
This is me…over here…feeling a cold burn which sometimes turns hot in my feet, but also sometimes my whole body. It’s been getting worse after taking a b-complex.
A friend of mine prompted me to research this. We have similar burning sensations! People sharing their burdens leads to good. So share with me.
So…why does supplemental B6 hurt some people but not others? Some people can get B6 toxicity related nerve damage while others can get B6 deficiency nerve damage. I propose that it all depends on the status of your NAD.
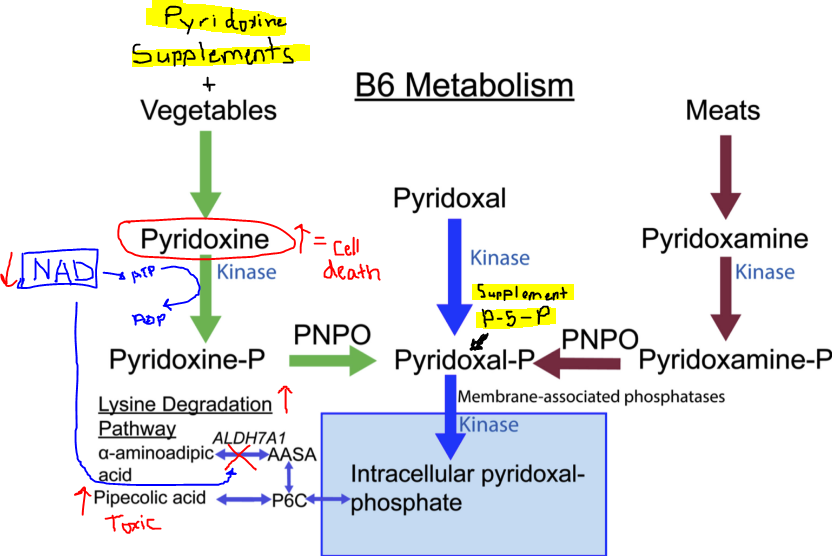
So if you start in a low NAD state, and use high dose B6, it might be problematic. Probably you have to avoid things that lower NAD before starting to supplement with B6 because in a round about way you have to have enough NAD to make ATP in the TCA cycle. ATP is needed to metabolize pyridoxine. Excess pyridoxine is toxic. (1)
To add to the complication, you need some B6 to make NAD! So avoiding B6 all together won’t help.
If your NAD is low, you won’t be able to run the ALDH enzyme in the picture on the bottom left. It could be that inability of B6 to be pushed towards Lysine production results in making a toxic metabolite called Pipecolic acid (2).
Excess pipecolic acid was found in a child with mutations in the ADLH7A1 gene who had seizure disorder. The solution for them was to restrict dietary lysine and supplement with B6 (3) which helped to restore normal levels of pipecolic acid. This was probably because lowering dietary lysine allowed for excess B6 to be shuttled towards Lysine production instead of pipecolic acid production. So interesting!
So, I propose that people with low NAD status are having similar situation. They are high in either unmetabolized pyridoxine from supplements or vegetables. This becomes toxic. OR they are high in pipecolic acid due to impaired NAD levels leading to the inability to convert any form of excess B6 into Lysine.
And I propose that the only way to safely detoxify excessive B6 is through pushing it into the amino acid lysine. To do this you have to not be impairing your NAD levels. So that means….
- no alcohol
- no excessive aldehydes from sodas
- no kombucha
- no excessive amounts of fermented products
- definitely don’t have a thiamine deficiency
- avoid oxalate like the plague
- don’t supplement with vitamin A (if you aren’t actually deficient) because that also requires NAD for processing
So if someone thinks that they have neuropathy from B6 toxicity maybe a low lysine diet would be beneficial? Here is a website that my friend shared with me. I’m so thankful for him. I haven’t really looked it over yet, because I really like science-ing things out in my brain first before I get opinions from other people. I definitely like input from other people because I’m not a know-it-all, but I always like to wrap my brain around a situation before I start to get input from various sources.https://understandingb6toxicity.com/…/small-fiber…/
Here is a side note…If someone is on hydrocortisone therapy, it can lead to what looks like a B6 deficiency on labs (high lysine, high tryptophan, low glutaric acid), but in actuality the steroid has impaired the Kyneurine pathway of NAD metabolism by inhibiting the enzyme TDO. See a post here regarding that.
What can I do for me and for my clients:
1. Only supplement thiamine at a high dose (and I’m still researching this…check out www.hormonesmatter.com for more info on high dose thiamine).
2. Keep B6 low at the RDA (or at least not at the level in most B-complex supplements). unless I know someone is deficient base on labs and history of B6 depleting medications such as seizure meds or birth control. Then possibly just give small doses but not excessive. ***** Avoiding high levels may be super important in people who can’t give up their NAD lowering habits – oxalate, metformin, alcohol, miralax, melatonin, etc.****
3. I’m NOT going to eat a lysine restricted diet because I don’t have a genetic mutation in ALDH7A1. I won’t make my clients do this either, unless they think they are toxic, because diet restriction of amino acids is too hard. If they do have this genetic mutation, though, I would. OR if they have symptoms of B6 toxicity I might recommend it.
4. Instead, work on sparing NAD because that is potentially what is causing the high pyridoxine or pipecolic acid. Low NAD may actually decrease ALDH7A1 activity. And…get this…people with liver disease have high Pipecolic acid levels. So…low NAD seen in oxalate poisoning and chronic alcohol issues leads to liver disease eventually. (4).
It’s all interconnected. How does vitamin A play into this? Excess retinol and retinal metabolism might deplete NAD in the same way. Once levels are high because of low NAD state, the vitamin A itself becomes a potential way that NAD levels are lowered. A vicious cycle.
There are no perfect solutions in nutrition and metabolism. Only trade offs. Maranatha.
(1) https://pubmed.ncbi.nlm.nih.gov/28716455/
(2) https://www.sciencedirect.com/…/medicine…/pipecolic-acid
(3) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9448604/
(4) https://aasldpubs.onlinelibrary.wiley.com/…/hep.1840080216
I’m a dietitian. Not a doctor. Talk with your doctor or personal healthcare practitioner before you make any changes to your diet, supplements, medications, or lifestyle. This is only meant to inform, not to treat or diagnose a condition.