
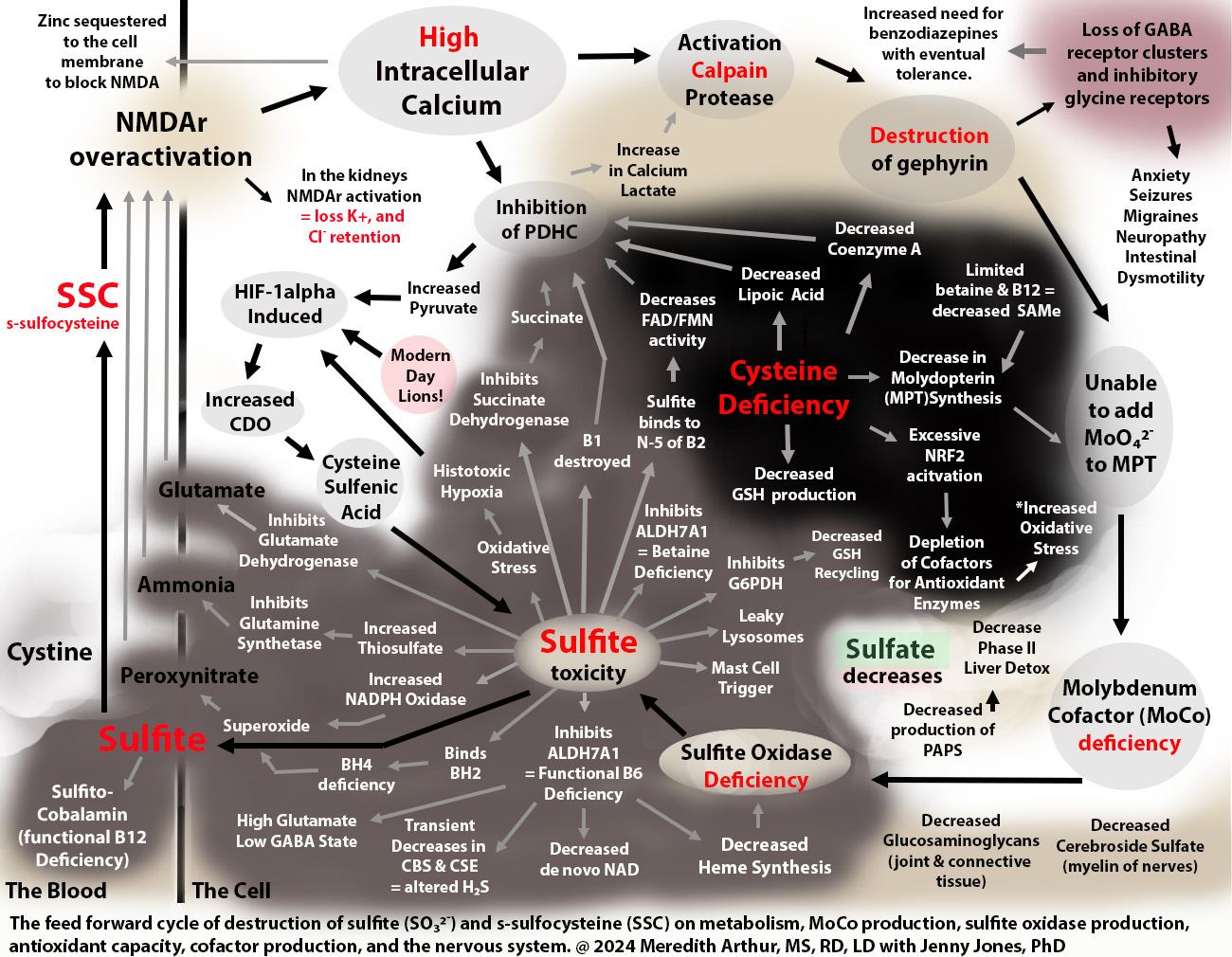
Sulfite toxicity and cysteine deficiency collide at the crossroads of transsulfuration and the HIF-1alpha pathway.
I’m a dietitian, not a doctor. This isn’t medical advice. Talk with your healthcare provider before making changes to your diet, supplements, medication, or lifestyle.
For the past year or so Jenny Jones and I have been discussing her MoCo Steal Theory. Her theory is that due to blocks in NAD recycling and various other blocks at ALDH, she had to use more of the low affinity, high-capacity enzyme for vitamin A metabolism, aldehyde oxidase (AOX). This caused a stealing of molybdenum cofactor towards AOX and away from sulfite oxidase (SO or SUOX) leading to a loss of sulfite oxidase activity. Sulfite then caused the functional B6 deficiency that she and I collaborated on where the moonlighting enzyme ALDH7A1 was completely inhibited by sulfite causing a sort of late-onset pyridoxine-dependent epilepsy from a functional B6 deficiency.
.
Controlling glutamate is important through dietary interventions to reduce free glutamate if you struggle with seizures or migraines, but there is a sneaky glutamate-like compound being made in our bodies every day called s-sulfocysteine (SSC). It’s the dipeptide cystine bound to free sulfite. Chris Masterjohn talks of how we all have this in varying amounts.
.
Jenny, Andrew Baird, Michelle Harris, and I have been discussing that vitamin A “toxicity” is actually vitamin A “dysregulation” and overall isn’t a poisoning from retinoic acid because most of us aren’t even getting to the point of making retinoic acid due to the massive dysfunction caused by sulfite toxicity.
.
After many months of research, I have concluded that Jenny’s MoCo Steal may have happened to some of my clients in the past including my daughter. However, I noticed that they had gone beyond a MoCo Steal and had fallen into a Sulfite Trap because when we can’t metabolize sulfite, we make s-sulfocysteine (SSC) and have excess free sulfite causing damage to our mitochondria leading to a feedforward cycle of destruction that meets at the crossroads of transsulfuration and the immune and hypoxia response pathway, hypoxia-inducible factor-1 alpha (HIF-1alpha).
.
Regarding vitamin A metabolism. SSC over-activates NMDA receptors on many cells in the bodycausing large increases in intracellular calcium which then causes retinol to efflux out of cells back onto RPB4. This is the high serum A that we experience. It’s a cellular deficiency of vitamin A, but blood toxicity.
.
Although high liver vitamin A stores are still possible, I think that high serum vitamin A is the squeaking wheel on a very broken race car called Acquired Sulfite Oxidase Deficiency. This leads to intolerance to vitamin A-rich foods. The thesis linked to in the description section of the video will explain dry skin, collagen loss, and poor glucuronidation, but this is not covered in this preliminary video below which only explains how we get trapped in this pathway.
But the damage doesn’t stop at vitamin A intolerance.
Both sulfite in the mitochondria and SSC cause an increase in the activity of cysteine dioxygenase (CDO) through the activation of HIF-1alpha. Upregulation of CDO leads to shutdown of the cells through s-sulfenylation with cysteine sulfenic acid. This is a life-saving effort to protect enzymes from oxidative stress so that when the cell turns back on, the cell won’t have to start all over again. The bad part is, that leftover cysteine sulfenic acid is metabolized to sulfite and should be further metabolized to the beautiful, life-saving sulfate which is used for Phase II liver detox. Instead, we make more sulfite which leads to more mitochondrial damage as well as more SSC which causes more increases in CDO and more sulfite. It’s a trap.
.
SSC itself causes alterations in metabolism that cause the loss of the ability to make MoCo because it leads to loss of gephyrin needed to add molybdenum to molybdopterin and eventually loss of the ability to make the SUOX enzyme as well for some people. Cells outside of the central nervous system express NMDA receptors, which can respond to SSC, including hepatocytes, a major site of sulfite oxidase activity.
.
This pathway leads to cysteine deficiency from tying up cystine in the blood with sulfite. This eventually leads to the inability to make FAD due to FAD synthase needs the cofactor molybdopterin (MPT) which requires a sulfur group from cysteine. MPT is NOT molybdenum. It’s the step before molybdenum. Taking molybdenum is not a way to restore FAD synthesis. It’s not involved in that reaction. Just MPT, the empty shell of MoCo, for lack of better terms, is what is needed for making FAD.
.
And the damage to other cofactors and pathways is evident. Anything that requires cysteine will be decreased such as lipoic acid, coenzyme A, activation of NRF2, and production of CoQ10 (although I mostly see this pathway conserved, if not high on Genova testing, because people need CoQ10 for the HIF-1alpha pathway, but they aren’t using it in their mitochondria at SQR as the mitochondria are shut down trying to repair the damage from sulfite and I doubt that CBS and CSE are working much at all due to functional B6 deficiency from sulfite inhibiting ALDH7A1).
.
Activation of NMDA receptors in the kidneys causes potassium wasting and sodium wasting, but chloride retention, and inability to uptake bicarbonate from urine lead to non-anion gap acidosis which is often missed by doctors. It can also cause hyperaldosteronism and hypertension. I suspect that anyone requiring high dose thiamine for life with high dose potassium intake is a maker of excessive amounts of SSC. Free sulfite is probably the cause of many individuals’ thiamine deficiencies as sulfite cleaves thiamine at the methylene bridge essentially destroying it.
.
In the brain, SSC over-activates NMDA receptors on GABAergic synapses leading to excessive calcium influx into cells, loss of gephyrin needed to hold GABA receptors in place, and destruction of the synapses. This leads to a high excitatory state with low inhibition and can cause seizures as well as anxiety, pain, bowel dysmotility, tremors, and dysautonomia.
.So…I humbly ask for you to consider this hypothesis that I’m living out in real time. I am not trying to be a savior. I’m just sharing an awful experience and showing my love for my fellow humanity by putting this out there. I am currently stuck in the sulfite trap with my daughter, Zoey. I got here when I took garlic and NAC to lower my blood pressure and then added in rolled oats. It was a snowball effect leading to severe sulfite toxicity. I think I have a way of escaping, but I am tired.
Because of the underlying sympathetic surges that I have right now, negative comments will harm me physically. Please refrain from making negative comments about Jenny and my work until you have thoroughly investigated it and proven it wrong. I would like for all the great minds out there in our world to take over and help find a solution to this problem if they feel that my hypothesis is valid. I think I have a few good ideas, but I do not know everything. I need YOU…smart people. Help save my brain and everyone else’s, please.
,
If I am wrong on this HYPOTHESIS. I may end up on 20 medications to control the massive symptoms that I have. However, currently, Benadryl is helping. This is not a medication recommendation for anyone…you MUST go to your doctor or practitioner with this idea. This is a dangerous trap.
Benadryl blocks NMDA receptors nicely and is reducing all my symptoms, but I’m still not fixed because when I stop the Benadryl, I fall back into horrible symptoms such as anxiety, tachycardia, insomnia, high blood pressure (some have low blood pressure), pain, internal tremors, burning sensation all over my body, and more. Only time will tell if blocking NMDA digs me out of the trap. I have a few other ideas as well in the collaborative thesis paper that Jenny and I worked on.
If you aren’t having a hypertensive crisis, there is another way out. I had a client heal with a few small changes. She still has migraines and histamine reactions, but her neurological symptoms have improved immensely. More on that soon.
CAUTION!!!!!!
Do not try to get out of this trap alone!!! Blocking NMDA restarts metabolism and some things might happen that aren’t pleasant. If you over block NMDA and then remove the block, you could have a SEIZURE. You must be aware of this risk. PLEASE WORK WITH YOUR PRACTITIONER.
Do not add NAC if you think you are stuck in this pathway until you get with a practitioner to find some way to block your NMDA receptor UNDER the SUPERVISION OF A HEALTHCARE PRACTITIONER but titrate it for your own needs and monitor your electrolytes and labs. Blocking NMDA receptors restarts metabolism, but we don’t have all the co-factors ready and I’m worried that fragile people need close monitoring. There is a risk that you don’t have all the cofactors for finishing the conversion from pyruvate to acetyl CoA. I think that this can lead to mitochondrial aldehyde toxicity. I sent a message to Dr Marrs about this. She plans to look at what I wrote on Monday.
I think whenever we’re using an NMDA blocker, UNDER SUPERVISION OF A HEALTHCARE PRACTITIONER we have to do a very gentle diet where we consistently eat only a small amount of carbohydrates every 2 to 2.5 hours so that we don’t go into full-blown lactic acidosis because lactic acidosis will get us stuck in the same pathway. Lactic acidosis could lead to the same increase in the CDO activity that I described in the video. So, it would be a low carbohydrate diet but not carbohydrate-free because to avoid gluconeogenesis as making glucose uses GTP. GTP is needed for making MPT and molybdenum cofactor.
Here is a link to the video. Here is a link to a HYPOTHESIS paper.
********************************