
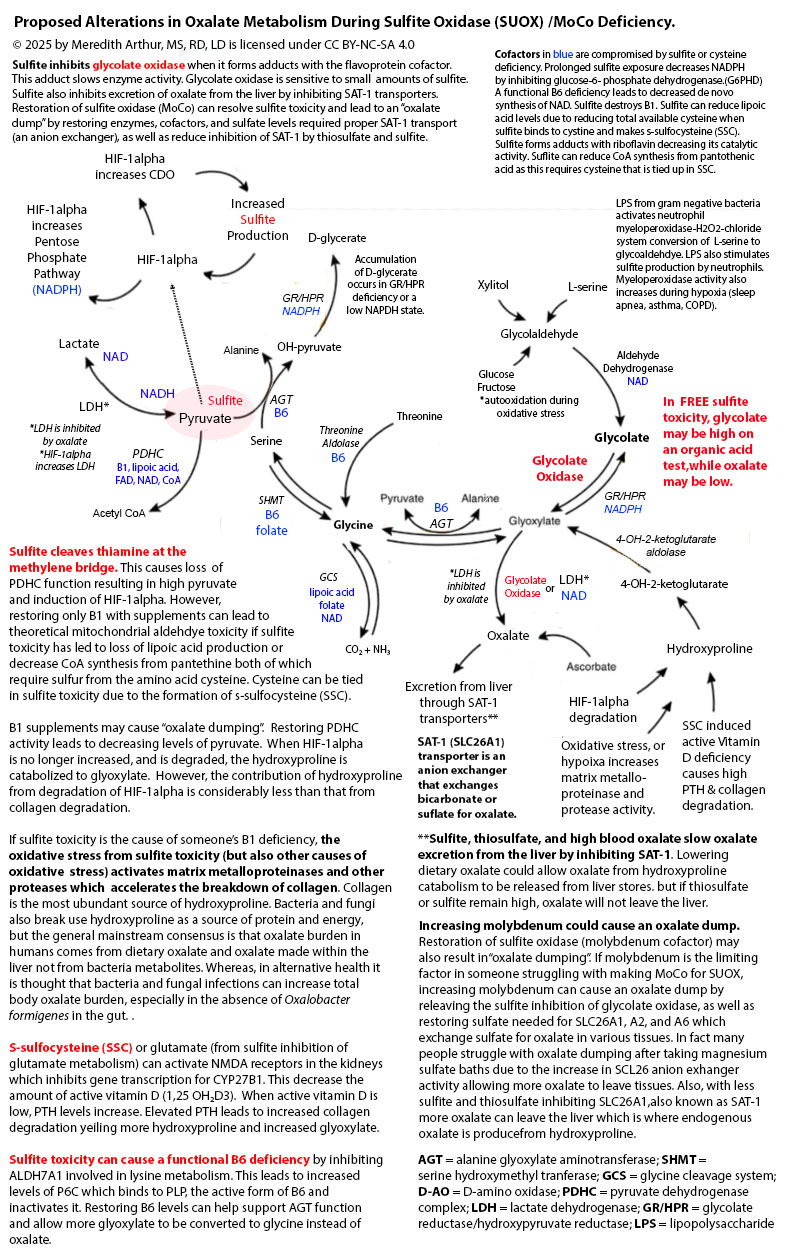
Zoey’s suddenly “cured” of hyperoxaluria as well as hyperuricemia. Is this a good thing? I think not. She has elevated glycolate levels, but low oxalate levels on her organic acid test, and her 24-hour urine oxalate levels are below the standard for someone her age as well as her urinary sulfate levels. I suspect worsening sulfite toxicity as the cause of her decreased glycolate to oxidase conversion. This isn’t a sign of improvement. It’s a sign of severe dysfunction. See the diagram below. Glycolate oxidase is inhibited by sulfite.
Zoey struggles with sleep apnea. Despite our best efforts, she rarely keeps her mask on for more than 2-3 hours per night. This means that during the night, her body increases gene transcription for HIF-1alpha in response to hypoxia. In a hypoxia state, HIF-1alpha goes to the nucleus and alters metabolism, including increasing the enzyme cysteine dioxygenase. This leads to a downstream increase in sulfite production which puts a burden on sulfite oxidase, the enzyme that metabolizes sulfite to sulfate. In addition, sleep apnea increases the activity of the enzyme xanthine oxidase. This used to be the cause of Zoey’s high uric acid levels. Xanthine oxidase uses molybdenum cofactor. Overall, sleep apnea sets the stage for Jenny Jones, PhD’s “Moco Steal” by increasing the need for more molybdenum for xanthine oxidase as well as increasing the total amount of sulfite produced by increasing CDO activity.
When the MoCo Steal from sleep apnea became extreme to the point that there wasn’t adequate molybdenum cofactor for sulfite oxidase, the sudden surge in sulfite caused a functional B6 deficiency through inhibition of ALDH7A1 resulting in a build-up of P6C. This led to decreased activity of cystathionine-beta synthase and cystathionine-gamma lyase. These two enzymes provide a significant amount of hydrogen sulfide that turns off the HIF-1alpha gene transcription. As hydrogen sulfide production decreased in Zoey’s enterocytes, she developed small intestinal bacteria overgrowth to compensate for the decrease in H2S (Greg Nigh has a theory that we grow sulfur metabolizing bacteria to provide our bodies what we need).
With the excess hydrogen sulfide in her gut, and a very oxalate restricted diet due to a history of hyperoxaluria, Zoey’s total molybdenum absorption decreased significantly due to sulfur can bind to molybdenum and when complexed with dietary copper, form a molybdenum-copper-sulfate complex that is unabsorbable. This perpetuated the problem. Over a year, her body became severely molybdenum cofactor deficient to the point that sulfite in her liver inhibited glycolate oxidase resulting in markedly high glycolate levels on her organic acids, but within range values of oxalate and below level oxalate on her 24-hour urine test.


Above you can see that Zoey’s 24-hour calcium levels have come down. She actually has decreased hypercalcemia because overall, she has improved from a vitamin A standpoint. Her serum vitamin A has dropped to 49 ug/dl which decreases osteoclasts being aggravated and breaking down bone.
Her 24 hour citrate levels have plummeted further. This is because sulfite can bind to pyruvate and prevent pyruvate metabolism to acetyl CoA. In addition, sulfite can damage all of the cofactors needed for the pyruvate dehydrogenase complex (B1, FAD, NAD, lipoic acid, and CoA). In addition, if sulfite is bound to pyruvate, it can’t be made into oxaloacetate. This leads to decreased overall levels of citrate.
Zoey’s urinary pH is quite neutral, but this is of concern to me because her blood chemistry panels over the past two years have shown hyperchloremic normal anion gap acidosis. This is consistent with renal tubular acidosis OR the actions of glutamate/s-sulfocysteine on NMDA in the kidney and activation of the sodium exchanger (ENaC). I have seen this hyperchloremic normal anion gap acidosis in many people who have suspected sulfite oxidase/moco deficiency. Activation of the ENaC results in uptake of sodium and chloride and wasting of potassium (sodium and chloride in urine below the reference range). Zoey’s urinary potassium is quite low, but her blood potassium is also low on blood draws. She has become potassium deficient and so her body is attempting to retain as much potassium as possible. During this 24-hour urine test she was getting 1000 mg of potassium citrate and 350 mg of magnesium citrate.
Zoey’s low phosphorous level is of a concern due to it may indicate intestinal malabsorption. She has a high risk for Crohn’s disease due to MBD5 deletion can increase the mRNA expression of FOLH1, that is higher in individuals with Crohn’s. The drop in her urinary sulfate below normal is consistent with sulfite oxidase deficiency. I suspect her levels are even lower because I give her magnesium sulfate foot baths every other day. The drop in her creatinine and urinary urea nitrogen indicated struggles with creatinine production (functional B6 deficiency and/or methylation decreased due to sulfite binding to B12, inhibiting betaine production, and oxidative stress damaging 5-methylfolate). Her low urinary urea nitrogen indicates a probable decrease in ornithine production needed for running the urea cycle as this is a byproduct of creatine production as well as can be made from proline but requires vitamin B6.
As you can see above, overall, Zoey is struggling with sulfite toxicity. I think that since birth (she had hypoxia in the womb due to placental abruption) Zoey has been stuck in the HIF-1alpha pathway to varying degrees her whole life. We are working on a therapeutic plan to deal with this constant, chronic uptick in sulfite production as well as strategic avoidance of sulfur foods at the time of taking mozyme forte.
References:
- Ghanem, Mahmoud. On the mechanistic roles of the protein positive charge close to the N(1)flavin locus in choline oxidase.
- Meier, Sebastian & Solodovnikova, Natalia & Jensen, Pernille & Wendland, Jürgen. (2012). Sulfite Action in Glycolytic Inhibition: In Vivo Real-Time Observation by Hyperpolarized 13C NMR Spectroscopy. Chembiochem : a European journal of chemical biology. 13. 2265-9. 10.1002/cbic.201200450.
- Oxidative stress from sulfite toxicity leads to loss of 5-methylfolate leading to burden on folate metabolism. Sulfite can bind to BH2 causing loss of BH4. Sulfite can lead to low levels of PLP. Pyridoxal 5’‐phosphate in cerebrospinal fluid; factors affecting concentration – Footitt – 2011 – Journal of Inherited Metabolic Disease – Wiley Online Library
- Glycolate Oxidase Is a Safe and Efficient Target for Substrate Reduction Therapy in a Mouse Model of Primary Hyperoxaluria Type I – ScienceDirect