
What if periodic “oxalate dumping”, intolerance to dietary oxalate, and subsequent low NAD/NADH ratio leading to hypervitaminosis A (retinol/retinaldehyde toxicity with simultaneous retinoic acid deficiency) is caused by a block at pyruvate dehydrogenase complex (PDHC) due to sleep apnea or due to the immune system activation during a fight against fungal infections or bacterial infections? What if lack of oxalobacter formigenes (breaks down oxalate) isn’t the only issue? What if gut dysbiosis triggers our own body to produce oxalic acid?
***I’m a dietitian and not a doctor. This post is written for informational purposes only and not meant as medical advice. Any therapeutic suggestions made in this post should be discussed with your own personal health care provider prior to making any changes to your diet, nutrition, supplements, or lifestyle.***
August 4, 2024 Meredith Arthur Leave a comment
On August 6th, 2023 I wrote this article Oxalate: A Potential Contributor to Hypervitaminosis A – Hormones Matter for hormone matter regarding a hypothesis that hyperoxaluria and high dietary oxalate contributes to hypervitaminosis A by altering cellular NAD to NADH ratio contributing to a high retinol state and a low retinoic acid state. I felt like dietary oxalate was a huge component to Zoey’s chronic hyperoxaluria and do believe that plantain flour, recommended by a dietitian who is an expert in kidney disease, was the cause of Zoey’s unfortunate oxalate poisoning. However, what if the reason that Zoey is unable to tolerate dietary oxalate is actually that she, herself, is an over producer of oxalate in her body depending on her oxygen levels or immune function?
Hypothesis: The cause of new onset idiopathic hyperoxaluria and glycolate toxicity may actually be overactivation of HIF-1alpha due to fighting bacteria, fungus, hypoxic conditions, and/or sleep apnea.
My daughter Zoey is unable to tolerate more than 50 mg of oxalate a day and is sick every afternoon with headache and nausea. Why? Although she lacks the genetics for primary hyperoxaluria, she periodically becomes an oxalate producer that at first seemed random. She also struggles with high glycolate levels on her organic acid test despite doing all the right things recommended for resolution of glycolate toxicity. Looking back on her twelve years of life, I have realized that her bouts of high urinary oxalate levels and horrible headaches weren’t random at all, but occurred when she was fighting a bacterial or fungal infection or when she was non-compliant with her CPAP mask for sleep apnea.
Recently this all worsened, and many of my side clients were experiencing similar issues. This prompted me to find an answer to this mystery. I asked myself, “What if hyperoxaluria, despite consuming a low oxalate diet, and having no genetic aberrations to cause hyperoxaluria, isn’t the product of bad glycine metabolism? What if it is the after effect or the ongoing effect of the activation of HIF-1alpha, a factor that is made in the body whenever it is fighting fungus or bacteria or when experiencing hypoxia?”
HIF-1alpha causes a block at pyruvate dehydrogenase complex (PDHC). After extensive research and comparing of organic acid test results among those who share them with me, I believe that a block at PDHC by HIF-1alpha may be the number one contributing factor to production of endogenous oxalate in the setting of B6 sufficiency, and this block at PDHC can account for a paradoxical reaction to B6 supplementation increasing oxalate formation. In fact, when people are functionally or marginally deficient to severely deficient in B6 I propose that they will make less oxalate while producing more glycolate, which unfortunately poisons them if the kidneys cannot keep up with excretion of this metabolite.
HOW DOES A BUILD UP OF PYRUVATE CAUSE HYPEROXALURIA?
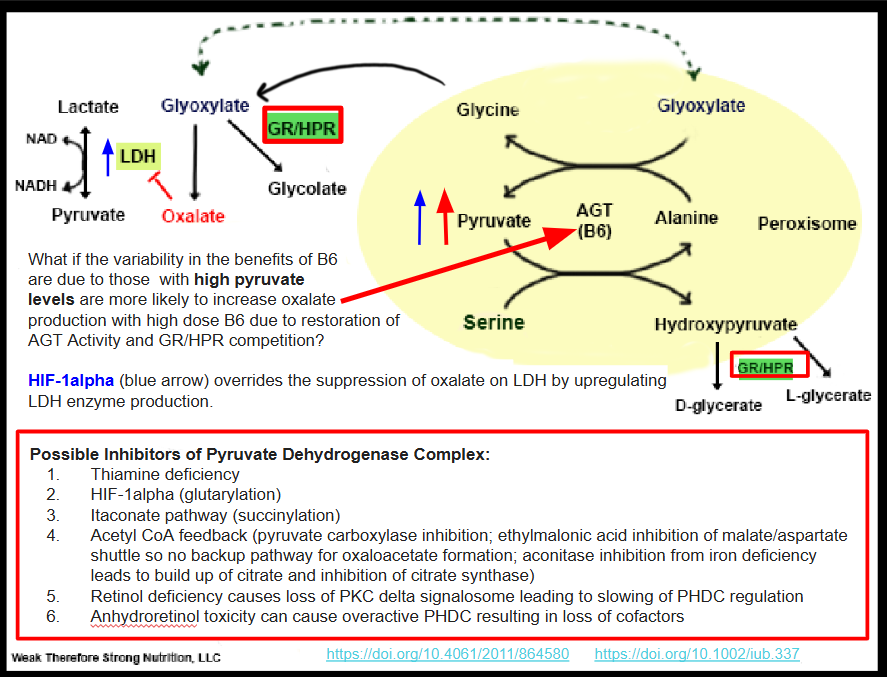
Pyruvate in excess that is unable to escape by six different metabolic pathways (explained further below) is shuttled to the peroxisome and combines with serine via a reaction metabolized by alanine glyoxylate transferase (AGT) to hydroxypyruvate (Figure 1). Hydroxypyruvate is then metabolized by Glyoxylate Reductase/Hydroxypyruvate Reductase (GR/HPR) to D-glycerate and L-glycerate. This enzyme is the same enzyme that metabolizes glyoxylate to glycolate. If this enzyme is tied up in hydroxypyruvate metabolism due to excess pyruvate build up, it may not metabolize glyoxylate to glycolate. The end result is more glyoxylate is made into oxalate via the enzyme lactate dehydrogenase (LDH). This should have feedback inhibition on LDH and stop the formation of further oxalates. However, if someone is fighting a bacterial or fungal infection, or even has excessive inflammatory macrophages produces excess NF-KB such as in the acute phase response to illness, HIF-1alpha increases. HIF-1alpha, in turn, upregulates the enzyme LDHA and so feedback inhibition by oxalate is overridden by the sheer abundance of lactate dehydrogenase available. LDHA is the same enzyme isoenzyme involved in glyoxylate to oxalate conversion and is actually a therapeutic target for individuals with primary hyperoxaluria. See Figure 1 for a pictorial demonstration of this pathway and a summary of inhibitors of PDHC.
When I added B6 to my own family members regimen to stop oxalate production, they only worsened. Of course, B6 is necessary for many reactions in the body, but what if the worsening of oxalate formation from adding B6 is due to supporting the already overworking AGT enzyme and the tying up of the moonlighting GR/HPR enzyme in dealing with hydroxypyruvate? Perhaps dealing with the block in pyruvate metabolism is the better way to solve the problem?
HYPEROXALURIA DUE TO EXTENSION OF IMMUNE FUNCTION
Whether fighting a bacterial or fungal infection, HIF-1alpha gets involved in redirecting glucose metabolism to provide energy for T-cells of the immune system via alteration of metabolism including inhibition of PHDC. In the research area myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) community, Dr. Rob Phair working with Dr. Ron Davis have a theory that ME/CFS occurs when cells other than the immune system take on an immune pathway. These cells adopt the itaconate pathway. Dr. Fair’s Itaconate Pathway theory for ME/CFS makes sense from a clinical standpoint as more and more people are experiencing altered metabolism.
If cells outside of the immune system are now taking on immune function, and there is an increase in HIF-1alpha orchestrating a multi-cellular response in the liver and kidneys, then it’s possible that HIF-1alpha pathway itself becomes a source of excess pyruvate that can contribute to hydroxypyruvate competition for GR/HRP. In addition, HIF-1alpha itself is tagged with hydroxyproline for degradation by proteasomes, and hydroxyproline can be a source of oxalate formation in PH type 1, 2 and 3 according to this in vivo human study. Overall, it appears that the adoption of a HIF-1alpha change in energy metabolism could be a major contributor to hyperoxaluria. My own daughter has experienced hyperoxaluria without having any genetic discrepancies as a contributing factor. What she does have, though, is chronic candida, and chronic bacterial infections, as well as sleep apnea as contributors to overactivation of HIF-1alpha.
WHAT ACTUALLY IS BLOCKING PYRUVATE METABOLISM?
HIF-1alpha itself has been shown to block PDHC leading to a buildup of pyruvate. However, it isn’t the only cause of a block at PDHC. In figure 1, I list the possible blocks of PDHC. Of course, thiamine deficiency is an obvious cause of loss of PDHC function and Dr. Londsdale and Dr. Marrs are the authorities on the downstream effects of thiamine deficiency. Yet, there are some people not responding to thiamine supplementation. These are the outliers. These are a few of the people in my family and some of my clients who do not improve with high dose thiamine, and possibly some of the people that I interact with online in forums who aren’t responding to thiamine supplementation. It may be that although thiamine can definitely fix the PDHC complex, along with other cofactors, it may or may not fix a metabolic block caused by the immune system or hypoxia. One question to explore would be, “If thiamine over-rides a metabolic block produced by the immune system, will bacteria and fungus be successfully eradicated?”
The lack of improvement with supplemental thiamine may be because HIF-1alpha causes a block at the enzyme pyruvate dehydrogenase complex (PDHC) leading to a buildup of pyruvate that must be shuttled somewhere. Figure 2, adapted from the six metabolic fates of pyruvate shows various ways that the cell deals with excess pyruvate. The seventh possible place for pyruvate to be shuttled is the peroxisome to form hydroxypyruvate as I show in Figure 1.
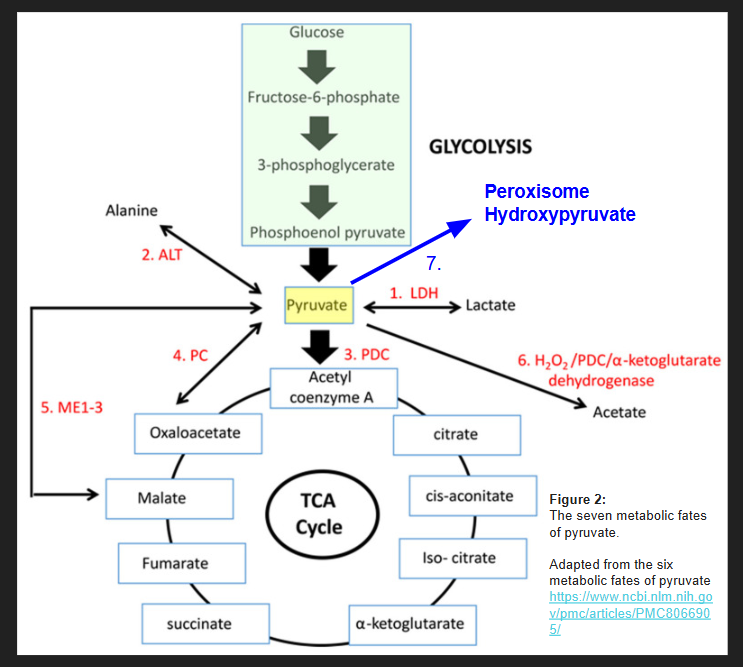
So, it’s possible that as long as there aren’t any blocks in enzyme #1-6 shown in figure one, that a person will not actually push pyruvate to the peroxisome to make hydroxypyruvate despite a block at PDHC for various reasons. Hyperoxaluria from a block at PHDC only becomes a problem when these other escape pathways for pyruvate are shut down, or when lactate is unable to be cleared from the body due to uremia (such as that occurs in chronic kidney disease or an obstructed ureter that occurs in kidney stone formation).
DIVERSION OF PYRUVATE AWAY FROM THE PEROXISOME
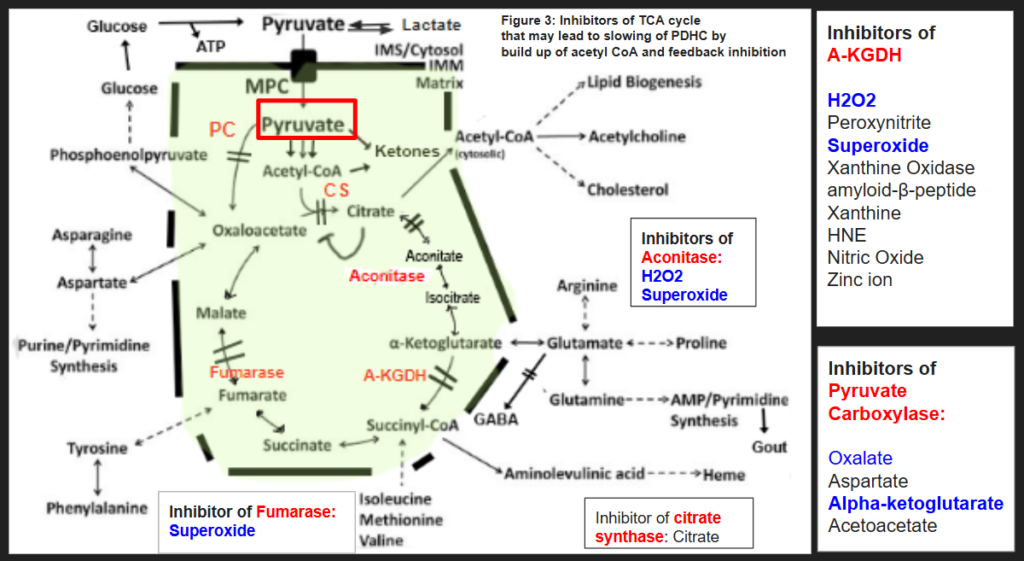
I think the goal of someone with hyperoxaluria who is stuck in a chronic state of fighting infection or struggling with hypoxia, is to concentrate on the six metabolic fates of pyruvate below. In figure 3, I have summarized some of the blocks of the enzymes of the TCA cycle that can lead to inhibition of pyruvate carboxylase and citrate synthase. Feel free to discuss these blocks with your own health care provider as I am unaware of your medical history. I hope to make a few short videos about how to get around each block in the pathways below in the future.
ORGANIC ACID TEST PROOF THAT BLOCKS AT PDHC CAUSE HYPEROXALURIA
Although I am currently taking a break from full time practice to care for my daughter, I often glance at organic acid tests for people who contact me and help them on the side, especially when someone has lost all hope. I have seen this trend of hyperoxaluria or high glycolate many times over in organic acid testing when someone is struggling with fighting a bacterial or fungal infection and has had to mount what seems to be a whole-body response. Here is a link to a recent YouTube video I have made that has screenshots of organic acid testing and explanations of how these results fit the picture of alterations in pyruvate metabolism contributing to hyperoxaluria. The video includes a little bit of theory on a sneaky metabolite of vitamin A, anhydroretinol, that could be causing some people to develop thiamine deficiency and also immune dysfunction leading to chronic infections that trigger chronic activation of HIF-1alpha.
HIF-1ALPHA DEGRADATION IN NORMOXIA CAUSES HYPEROXALURIA AND GLYCOLATE POISONING.
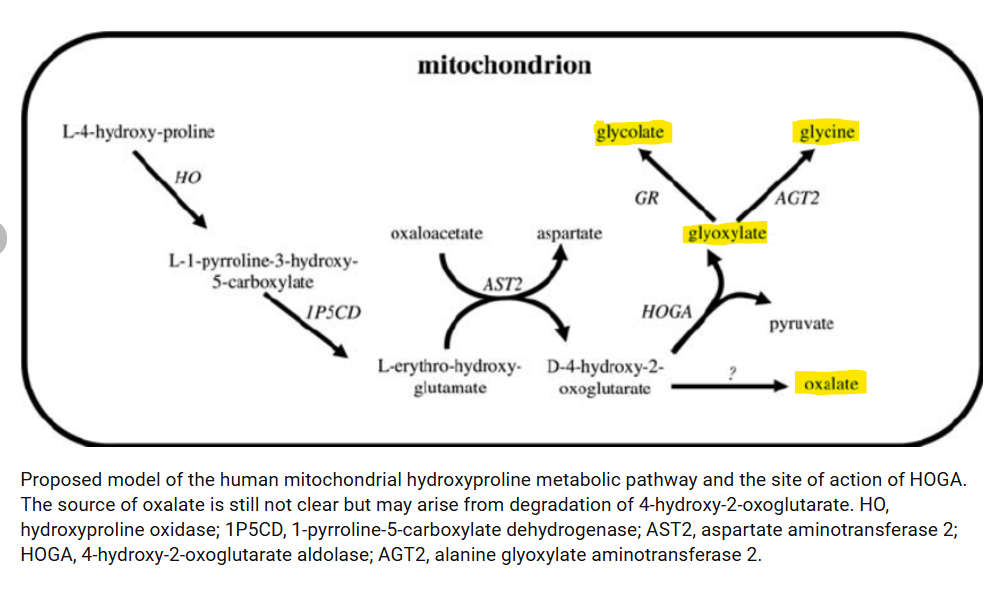
During a fungal infection in the absence of hypoxia, HIF-1alpha degradation will lead to increasing levels of hydroxyproline after it is ubiquitinated and degraded. This leads to an excess of hydroxyproline that must be metabolized as it is unable to be used again to synthesize proteins. This can lead to high oxalate formation as well as glycolate formation. This process can also happen in individuals with sleep apnea that can maintain normal oxygen levels while awake. These individuals cycle between low oxalate and glycolate states to high oxalate and glycolate states. In fact, Zoey, my daughter with sleep apnea, consistently has a headache and nausea every afternoon no matter what foods I feed her. She wakes up a bit sleepy, has a pretty good morning, and then goes downhill by the afternoon and requires Zofran for nausea and lays on the couch completely incapacitated. I believe this could be due to her body catching up with HIF-1alpha degradation with the resulting production of glycolate and oxalate. It appears she isn’t alone. Hydroxyproline degradation has been found to be a contributor to oxalate formation in all three types of primary hyperoxaluria. Perhaps the source of the excess hydroxyproline is overactivation of the HIF-1alpha pathway. Figure 4 shows that hydroxyproline is metabolized in the mitochondria to glyoxylate, glycolate, and glycine, and oxalate.
EVIDENCE THAT THIS IS TRULY HAPPENING? ORGANIC ACID TESTS FOUND IN VIDEO BELOW.
The video below goes through individual labs, and, in particular, shows one client who ate carnivore diet for about one week before her second organic acid test. This diet completely resolved her hyperoxaluria and high glycolate levels! This particular client’s information is at about 27 minutes and shows that changing to a very low carbohydrate diet alleviating her hyperoxaluria.
SOLUTIONS TO HIF-1ALPHA INDUCED HYPEROXALURIA?
Honestly, I have thought long and hard about this. My daughter Zoey has moderate to severe obstructive sleep apnea causing chronic hypoxia and induction of HIF-1alpha. I explored the possibility of inhibiting the gene transcription for HIF-1alpha with known inhibitors. I think for my own daughter, Zoey, I will not be trying to inhibit HIF-1alpha through use of known inhibitors. I believe that this could be counterproductive if she is fighting a fungal or bacterial infection.
However, I do plan on controlling her sleep apnea issues. She wears CPAP at night but is quite non-compliant with it. Her sleep medicine doctor is willing to try a little bit of oxygen, but we are also doing an evaluation with an ENT to make sure that her sinus passages are normal as well as an evaluation with neurosurgery because she has an alteration in her C1 vertebrae that could be causing the hypotonic sleep apnea. I highly recommend if someone has an underlying apnea issue, to have a CT scan of the sinus and C1 vertebrae. These areas, if altered, can be a major source of hypoxia.
Something else to consider is that fighting off pathogens causing high levels of reactive oxygen species (ROS) through NOX, but also sleep apnea itself induces the activity of an enzyme, xanthine oxidase, that also creates reactive oxygen species which inhibits proline hydroxylation of the pro-oxidative stress, HIF-1alpha. This keeps HIF-1alpha in an active state causing massive oxidative stress through NOX and down regulation of antioxidant HIF-2alpha. This type of high activity of NOX is pathogenic and can lead to excessive ROS and disease. How would someone know if they have elevated XO activity? They could monitor uric acid urine levels while eating carbohydrates and on a low purine diet (as purines will definitely increase uric acid alone). Xanthine oxidase converts xanthine to uric acid. Inhibitors of xanthine oxidase might be beneficial for people with chronic hypoxia to lower the overall oxidative stress on the body. Although drugs are available for this purpose, you might choose natural inhibitors of xanthine oxidase with your own healthcare provider.
Another goal that I have for my daughter, Zoey, is to avoid fungal and bacterial infections. This, of course, takes a bit more work from a nutrition standpoint. Definitely seek out a practitioner who understands the importance of nutrition for immune health as avoiding chronic fungal or bacterial infections is likely the key to prevention of extreme alterations in metabolism by HIF-1alpha expression. However, I do think having normal gene transcription for HIF-1alpha is crucial to mount a defense against pathogens.
Something I definitely don’t recommend if you have an active bacterial or fungal infection is a carnivore or keto diet long term. These diets may help with working around the block in metabolism at PDHC by lowering total glucose availability, but if there is truly an infection that needs to be resolved, a carbohydrate free diet will starve immune cells of very much needed glucose. Glucose is needed to fuel the HIF-1alpha upregulated pentose phosphate pathway to make NADPH which is used by NADPH dependent oxidase (NOX) to produce superoxide for killing pathogens. When I noticed that someone I am caring for has high microbial or fungal markers on their OAT, even though they might feel better on a keto diet because it lowers total pyruvate levels and decreases both glycolate and oxalate production, I think it would be better to continue to eat a well-balanced diet to fuel the immune system. They might realize that eating about 100 grams of carbohydrate per day is a happy medium where they don’t feel sick from glycolate and oxalate, but they are still able to maintain immune function. This would be per person of course.
Overall, I think discovery of this possible mechanism of increased oxalate and glycolate formation due to a block at PDHC from HIF-1alpha is going to change my daughter’s life. We have a new focus on how to promote her health and well being. The mystery of hyperoxaluria is not so much a mystery afterall.