This post is a work in progress! I actually hope to have a research lab that I know who is very interested in sleep disorders to help me out here.
What if sleep disorders are just impaired vitamin A metabolism?I constantly hear this from clients and patients, “When I eat “x” I can’t sleep.”
Zoey’s no sleep foods include: chocolate, beans, and french fries. These are all high oxalate foods. Oxalate is a potent inhibitor of LDH which lowers NAD recycling. Low NAD will prevent vitamin A metabolism to retinoic acid which is the “active” form of vitamin A in the body.
Luckily, Zoey never had plantain flour after noon. By the way, plantain flour is not low oxalate and this is what led to her current vitamin A toxicity issues. You can read the short story here, or for the long version you can head to
I am now convinced that we are cycling between retinol/retinal and retinoic acid throughout the day in various organs. I think that people who stay in a high retinol/retinal state have a risk of vitamin A toxicity.
If people have low NAD habits, they will have a high risk of toxicity, but even without toxicity, low NAD habits can lead to physiological low levels of retinoic acid in various organs.
I think we who are NAD compromised must compartmentalize. People with mitochondrial disorders definitely compartmentalize. They can’t have healthy skin AND sleep. They can’t have a normal immune system AND sleep. Then, when NAD is really low they can’t have any of these because there is no more retinoic acid to compartmentalize with.
Well, retinoic acid is a ligand for Retinoic Acid Related Orphan Receptors that code for many proteins that have various functions in the body including making circadian rhythm proteins. In a low NAD state we aren’t making retinoic acid in sufficient amounts. I see this with my own daughter and also with my clients. They have all the signs of vitamin A deficiency, but are actually vitamin A sufficient and many have hypervitaminosis A due to being in a low NAD state too long.
Circadian Rhythm Proteins!!! Zoey’s mouse model of MBD5 makes very low amounts of these. If you add in a functional vitamin A deficiency, retinoic acid deficiency, then….BAM…no sleep.
What if InZomnia (my nickname for Zoey’s sleep habits when they are disrupted) is actually poor retinoic acid production? I think it is.
How to win back sleep! The Solution?
First, if you aren’t vitamin A toxic, I would avoid high oxalate foods after 2PM daily.
If you are vitamin A toxic, you could still avoid high oxalate foods after 2PM daily, but be aware that you must fix your detox pathways before you start to mobilize more retinol/retinal to retinoic acid. Going low oxalate before you are able to detox high amounts of retinoic acid could be problematic. Read here for more information on this.
Getting 30 minutes of morning sunlight every morning without sunglasses to set the clock for triggering melatonin release. Melatonin isn’t the only circadian rhythm protein, but it is a big one. Avoid melatonin supplements. This impair vitamin A by lowering NAD+ and also using up NAD plus in metabolism. You can read more about that here.
Alternatively you can purchase a therapy light. I have a Verilux Happy Light that we use in our home.
Avoid blue light two hours before bed. You can buy glasses with blue blockers, or put your device in nighttime mode to decrease blue light.
Make your room COLD. It makes us want to stay under the covers. I’m sure it helps in other ways, but I haven’t researched this yet. Feel free to comment if you know more about this.
Establish a soothing bedtime routine. Perhaps a bath, a non-electronic book, and prayer, to get you in the sleepy mood you need to be in.
EGGS for sleep????
Eggs will help with sleep because a metabolite of cholesterol can be a ligand for ROR. Eggs are a good source of cholesterol. However, they also do contain vitamin A…that’s a whole controversy in the vitamin A detox world. The benefits of eggs, in my opinion, outweigh the risk. Eggs are a good source of phosphatidyl choline which is needed for the very last phase of liver detoxification when drug metabolites (and vitamin A metabolites) are excreted into bile for removal from the body. At the same time that bile salt is excreted, phosphatidyl choline also leaves the liver cells. Hypervitaminosis A places a huge burden on phosphatidyl choline needs and over medication can do this as well. We can add to that the need to metabolize environmental toxins, and it is easy to see that phosphatidyl choline is an under-rated nutrient.
Also, statins would be bad here because they lower cholesterol production. No amount of coenzyme Q10 restoration is going to replace the metabolites of cholesterol that are needed as ROR ligands. These effects could go beyond just sleep proteins as you can see in this article.
So…that’s about it. Good night, sleep tight, don’t let the NAD bugs bite!
This is not written to diagnose or treat a condition, but only for informative purposes. Please consult your doctor before stopping or starting medications or supplements, and before making dietary or lifestyle changes based on the information provided. – Meredith Arthur, MS, RD, LD
OXALATE from plants or made from VITAMIN C or GLYCINE or Miralax (PEG) in the body can impair Vitamin A metabolism
Oxalate is a component of plants that is impossible for the body to completely break down. It is a poison. We absorb it at variable rates, but some of us make it in our bodies from vitamin C and glycine. Excess vitamin C becomes oxalate through direct breakdown and without enzymes. Usually this occurs in vitamin C over 2000 mg, but it can happen at lower doses as well. Never take vitamin C to “bowel tolerance” as this is likely actually death of the intestinal cells due to oxalate poisoning. Glycine is metabolized to oxalate in a B6 and thiamine deficient state, but when there is adequate B6 and Thiamine, it does not become oxalate.
When oxalate is high it impairs an enzyme called Lactate Dehydrogenase (LDH). We have to make some lactate to keep energy metabolism going. When the body is producing lactate, it also produces NAD+ which is what drives vitamin A (retinol and retinal) metabolism forward. What I found through a deep dive into literature is that Oxalate doesn’t directly inhibit alcohol dehydrogenase or retinol dehydrogenase or aldehyde dehydrogenase which was what I was searching for. Oxalate actually impairs lactate dehydrogenase (LDH) which lower NAD+ levels. I hypothesize that oxalate takes away the “energy” needed to drive those reactions forward by impairing LDH.
LDH is actually the last enzyme involved in the formation of oxalates. I believe that oxalate being able to have a feedback inhibition on LDH is a safety mechanism built into our human biology, but that it backfires and wreaks metabolic havoc on vitamin A metabolism and also energy metabolism.
Oxalate impairs LDH activity via NAD dependent pathway
Oxalate Pathogenic In Autism (Perhaps this is the connection! If oxalate impairs LDH, resulting in low NAD, then retinal levels increase. These complex with ethanolamine causing A2E and microglial activation resulting in neurological decline. Read this post for more information.)
Jenny Jones, PhD, pointed the article below out to me as supporting evidence for the connection between need for normal LDH reaction to restore NAD levels. She is the oracle to my batman!
The article bleow is an excellent article! This gives the big picture of NAD production, recycling, and salvage pathways. Amazing! LDH, which is inhibited by oxalate, plays a pivotal role in NAD recycling.
NAD+ metabolism: pathophysiologic mechanisms and therapeutic potential
2. Avoid excess vitamin C in excess (variable per person, but most kids don’t need more than 500 mg per day)
3. Ensure adequate levels of B6 and thiamine (Seizure meds tend to deplete B6 – ask doctor about 50 mg of P5P, active form of B6) – ask doctor before starting supplements – CAUTION!!! I believe that supplementation of any form of B6 in a low NAD state will cause B6 toxicity. Read this post for that hypothesis.
4. Avoid glycine supplements and also collagen powders as these are high in glycine
5. Avoid Miralax or any PEG product (macrogol is another name for PEG) – see below
MIRALAX can become OXALATE and also can tie up alcohol dehydrogenase and dehydrogenase that are needed for Vitamin A metabolism
Approximately 3.7% of PEG based laxatives are absorbed. This can be metabolized by the body to glyoxylate and then to oxalate especially in a B6, Thiamine, or Niacin deficient state. This will impair LDH, subsequently lower NAD, and thus impair vitamin A metabolism, but also overall metabolism. In addition the first two steps of PEG metabolism involve alcohol dehydrogenase and aldehyde dehydrogenase. They are enzymes used in vitamin A metabolism. So Miralax may tie up these enzymes for an unknown period of time. This would be an interesting study in a rat lab.
So many people with Autism take PEG (Miralax). PEG can also cause gut dysbiosis (see below for info on bacterial steal of NAD+) Perhaps many have A2E complexes of the essential ether lipid ethanolamine due to increasing retinal levels (this is a hypothesis).
PEG with weights greater than 4000 aren’t absorbed (1960 studies), but somewhere along the way a manufacturer changed it out for PEG 3500, probably due to cost, and the researchers felt absorbing 200 ml out of 5400 ml was no big deal.
I propose that 3.7% absorbed of the PEG laxative are causing a big deal. And the unabsorbed product is causing gut dysbiosis.
Ever notice that the label says not for use in children? Also to not use more than a week?
2. Ask your doctor for alternatives such as magnesium, senna, glycerin suppositories, etc.
This is not written to diagnose or treat a condition, but only for informative purposes. Please consult your doctor before stopping or starting medications or supplements, and before making dietary or lifestyle changes based on the information provided. – Meredith Arthur, MS, RD, LD
I am a dietitian. I am not a doctor. This is not medical advice, but only written to inform. Please consult with your personal health care practitioner before starting or stopping supplements or medications, and before making any changes to your diet.
Simple Sum Up
Melatonin is known to help induce sleep
It often doesn’t keep us asleep because it is metabolized away in about four hours
High dose Melatonin (above 3 mg in children and above 5 mg in adults) is NOT good for the brain
Melatonin catabolism uses ADH and ALDH
ADH and ALDH are also enzymes that metabolize Vitamin A
Melatonin also inhibits TDO enzyme of the Kynurenine pathway
This stops the production of NAD in the liver, kidneys, and brain
NAD is a cofactor for the enzymes that metabolize vitamin A
High dose Melatonin will cause vitamin A to stay in its retinal/retinol form.
Excess retinal in the brain can bind to ethanolamine.
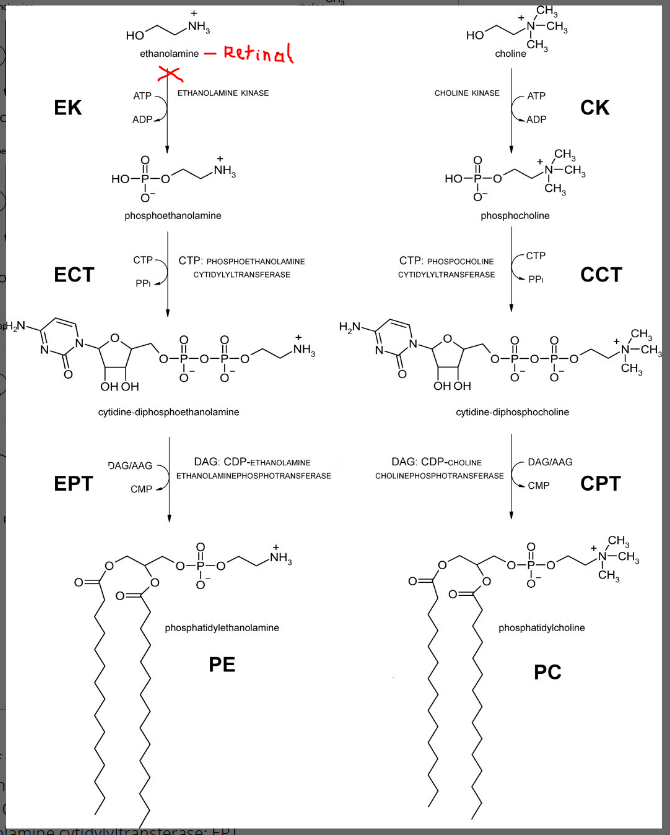
Phosphatidyl-ethanolamine is a precursor for choline synthesis.
Low choline levels leads to low acetylcholine which is the major neurotransmitter of the gut, brain, and heart (think slow gut, slow brain, slow heart.)
Also, when ethanolamine combines with retinal it can form A2E which is a schiffs base. This aggravates microglia cells which causes inflammation in the brain in my opinion. (Is my child drunk and also toxic on retinaldehyde?)
This post could pertain to adults who take more than 5 mg per day or to children taking more than 3 mg per day. Also anyone who doses melatonin multiple times a day, and anyone who has been on oral melatonin for quite some time may be at risk for all discussed below. Monitor yourself for symptoms of melatonin toxicity at the body of this article.
MELATONIN FOR SLEEP?
Melatonin is often prescribed to individuals with autism and intellectual disability because these people often struggle with sleep. In fact, the MBD5 deletion mouse model of Zoey’s genetic syndrome makes less circadian rhythm proteins in general. This leads to a predisposition for, what I like to call, InZomnia. We did give Zoey melatonin on and off for a few months when she was around two years old, but she would also have worse “drunk days” after taking melatonin. She would run into walls, so we stopped this supplement. I’m actually glad we did. We did have to learn how to promote better sleep hygiene in alternative ways. I think if we had kept using melatonin, she would have worse hypervitaminosis A than she does now.
The reason why Zoey was more “drunk” the day after taking melatonin is that high dose Melatonin actually alters NAD levels in the brain and also can compete with enzymes for alcohol and aldehyde metabolism. I will explain further….
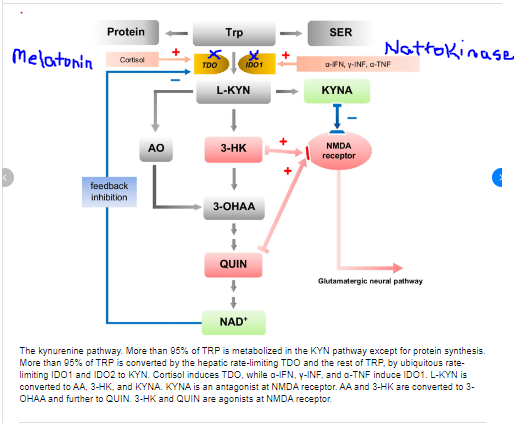
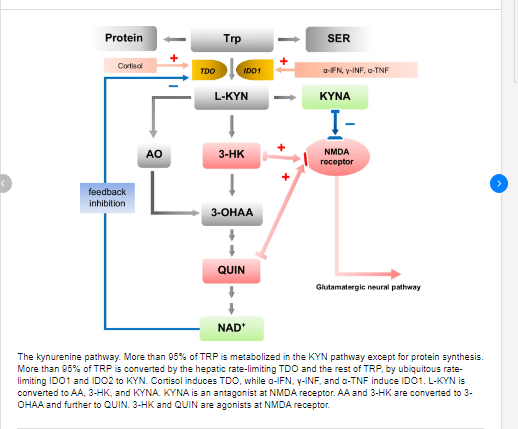
MELATONIN and the KYRURENINE PATHWAY
Figure take from this article and adapted https://www.researchgate.net/publication/339877327_Antidepressant-like_effects_of_kynurenic_acid_in_a_modified_forced_swim_test
High dose melatonin inhibits the enzyme TDO in the liver, brain, and kidney. This lowers NAD production. I believe this is in a dose dependent manner. The more melatonin given, the more this enzyme is blocked. The more often melatonin is dosed, the lower NAD production will be in these organs. This will cause higher amounts of retinol/retinal in these organs, and low levels of retinoic acid. Low levels of retinoic acid in the brain can alter nerve conduction by altering how many voltage gated calcium channels are open.
MELATONIN NEEDS ADH and ALDH FOR CATABOLISM
In addition, to actually blocking NAD production, melatonin may competitively impair retinol/retinal metabolism. Melatonin is metabolized using the enzymes alcohol dehydrogenase and aldehyde dehydrogenase. These enzymes are also used in vitamin A metabolism. Large doses of melatonin could compete with Vitamin A for metabolism resulting in a retinoic acid deficiency. Again, alterations in retinoic acid levels could contribute to changes in nerve conduction and either slow the brain down or speed it up by altering how many voltage gated calcium channels are open.
In addition, consider that if these enzymes in the brain are metabolizing melatonin, this could lead to higher levels of endogenously produced alcohols and aldehydes in the brain and could be the cause of the “drunk symptoms” that Zoey gets the morning after melatonin.
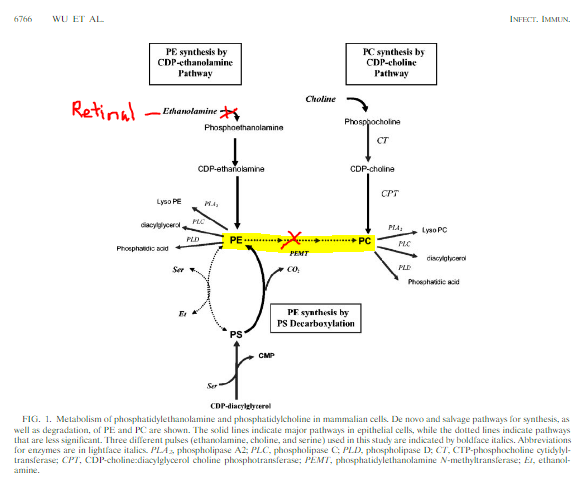
Adapted from ….https://journals.asm.org/doi/10.1128/IAI.72.12.6764-6772.2004
FURTHER CONSEQUENCES OF MELATONIN ALTERING VITAMIN A METABOLISM
The inability to convert retinol to retinoic acid in the liver leads to increased hepatic storage of retinol as retinyl esters which can lead to liver toxicity as well as a further burden on choline as it is needed for the enzyme Lecithin Retinol Acetyltransferase (LRAT) which helps to store vitamin A . (I will post soon about how low levels of retinoic acid in the kidney can cause kidney disease.)
High levels of retinal in the brain can complex with ethanolamine, an amino acid that is typically part of an important ether lipid that provides structure to the brain and helps it move smoothly. You can read more about how retinal and ethanolamine combine to form A2E, a schiffs base which aggravates microgrial cells resulting in brain inflammation and neurodegeneration here.
Adapted from https://iubmb.onlinelibrary.wiley.com/doi/10.1002/iub.337
Phosphatidyl-ethanolamine is actually a precursor choline synthesis as well, so in a round about way, melatonin is actually placing a huge burden on choline needs in the liver and the brain. Melatonin keeps retinal from becoming retinoic acid by altering NAD levels and also tying up ALDH in metabolism. This leads to high levels of retinal which can bind to ethanolamine. Low levels of phosphatidyl ethanolamine makes the body more reliant on dietary choline to produce phosphatidyl choline. More choline will be sequestered into the CPD-choline pathway shown below which means less choline is available for acetylcholine production (again…think slow gut, slow brain, and slow heart.)
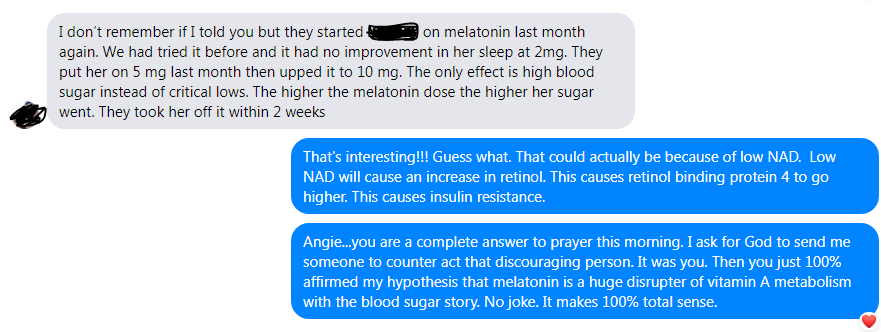
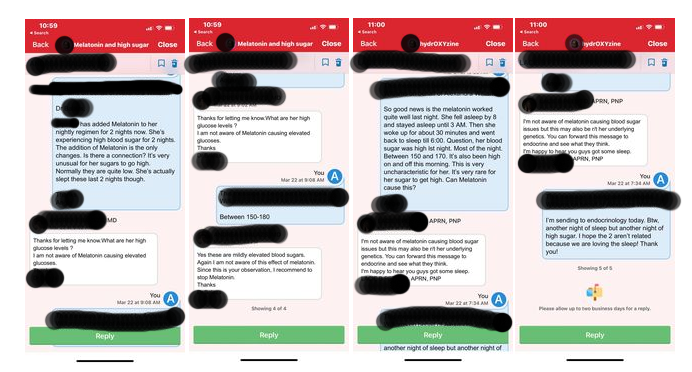
I have a friend in our 2q23.1 (MBD5) deletion support group who share a recent story of starting melatonin for sleep. As she increased her daughter’s dose of melatonin, there was a dose related response in blood glucose levels. As the dose went up, blood glucose levels went up. It is quite possible that as the dose increased, NAD levels decreased to the point that retinol levels increased, and retinoic acid levels decreased. High RBP4 can actually causes insulin resistance which would cause hyperglycemia (https://pubmed.ncbi.nlm.nih.gov/16034410/), and high retinoic acid can cause hypoglycemia (https://pubmed.ncbi.nlm.nih.gov/20032483/).
Here is our conversation….
And here is the conversation she had with different care providers about the high blood glucose from Melatonin.
WHAT IF THE SIDE EFFECTS OF MELATONIN OVERDOSE ARE ACTUALLY SIGNS OF RETINOIC ACID DEFICIENCY?
Alopecia and dermatological manifestations of melatonin overdose could actually be related to retinoic acid deficiency. In addition, when metabolizing large amounts of melatonin, NAD is used which may contribute to low cellular levels of NAD. This can result in impaired energy (ATP) levels leading to the symptoms described in melatonin overdose such as fatigue. This could also cause buildup of lactate resulting in lactic acidosis which would account for the vomiting seen in melatonin overdose.
Okay….so not to pull the “my child is more disabled than your child” card here, BUT the mouse model of MBD5 deletion doesn’t make very much circadian rhythm proteins. However, we got Zoey to sleep WITHOUT melatonin! Woohoo! If we can do it and genetics is playing a huge role against us, then you can do it too! How did we do it?
Sleep Hygiene.
Dark room
Cold room
Warm bath before bed
No screens (blue light) two hours before bed
Verilux happy light (or other light therapy light) in the morning for 30 minutes OR natural sunlight to trigger the timing of melatonin release for 12 hours later.
Prayers before bed. <3
Overall I do NOT recommend melatonin supplementation. The end.
This is me…over here…feeling a cold burn which sometimes turns hot in my feet, but also sometimes my whole body. It’s been getting worse after taking a b-complex.
A friend of mine prompted me to research this. We have similar burning sensations! People sharing their burdens leads to good. So share with me.
So…why does supplemental B6 hurt some people but not others? Some people can get B6 toxicity related nerve damage while others can get B6 deficiency nerve damage. I propose that it all depends on the status of your NAD.
adapted from https://www.pedneur.com/article/S0887-8994(17)30124-8/fulltext
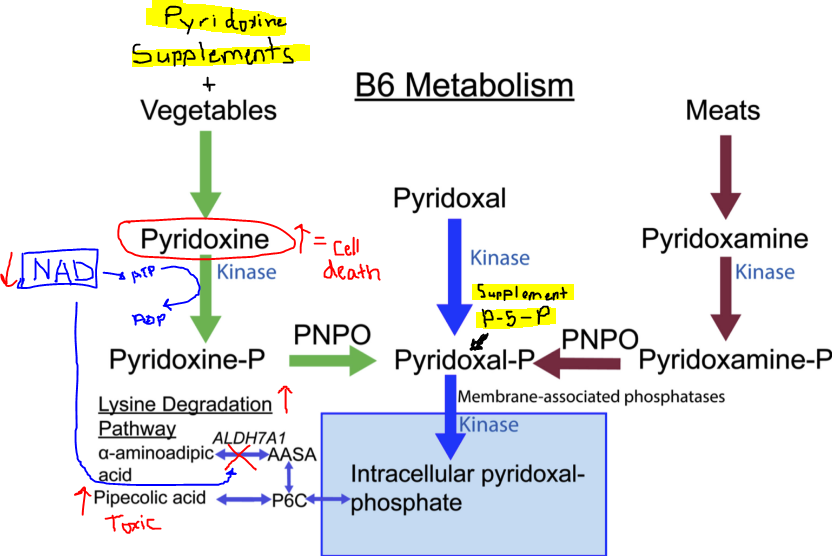
So if you start in a low NAD state, and use high dose B6, it might be problematic. Probably you have to avoid things that lower NAD before starting to supplement with B6 because in a round about way you have to have enough NAD to make ATP in the TCA cycle. ATP is needed to metabolize pyridoxine. Excess pyridoxine is toxic. (1)
To add to the complication, you need some B6 to make NAD! So avoiding B6 all together won’t help.
If your NAD is low, you won’t be able to run the ALDH enzyme in the picture on the bottom left. It could be that inability of B6 to be pushed towards Lysine production results in making a toxic metabolite called Pipecolic acid (2).
Excess pipecolic acid was found in a child with mutations in the ADLH7A1 gene who had seizure disorder. The solution for them was to restrict dietary lysine and supplement with B6 (3) which helped to restore normal levels of pipecolic acid. This was probably because lowering dietary lysine allowed for excess B6 to be shuttled towards Lysine production instead of pipecolic acid production. So interesting!
So, I propose that people with low NAD status are having similar situation. They are high in either unmetabolized pyridoxine from supplements or vegetables. This becomes toxic. OR they are high in pipecolic acid due to impaired NAD levels leading to the inability to convert any form of excess B6 into Lysine.
And I propose that the only way to safely detoxify excessive B6 is through pushing it into the amino acid lysine. To do this you have to not be impairing your NAD levels. So that means….
no alcohol
no excessive aldehydes from sodas
no kombucha
no excessive amounts of fermented products
definitely don’t have a thiamine deficiency
avoid oxalate like the plague
don’t supplement with vitamin A (if you aren’t actually deficient) because that also requires NAD for processing
So if someone thinks that they have neuropathy from B6 toxicity maybe a low lysine diet would be beneficial? Here is a website that my friend shared with me. I’m so thankful for him. I haven’t really looked it over yet, because I really like science-ing things out in my brain first before I get opinions from other people. I definitely like input from other people because I’m not a know-it-all, but I always like to wrap my brain around a situation before I start to get input from various sources.https://understandingb6toxicity.com/…/small-fiber…/
Here is a side note…If someone is on hydrocortisone therapy, it can lead to what looks like a B6 deficiency on labs (high lysine, high tryptophan, low glutaric acid), but in actuality the steroid has impaired the Kyneurine pathway of NAD metabolism by inhibiting the enzyme TDO. See a post here regarding that.
What can I do for me and for my clients:
1. Only supplement thiamine at a high dose (and I’m still researching this…check out www.hormonesmatter.com for more info on high dose thiamine).
2. Keep B6 low at the RDA (or at least not at the level in most B-complex supplements). unless I know someone is deficient base on labs and history of B6 depleting medications such as seizure meds or birth control. Then possibly just give small doses but not excessive. ***** Avoiding high levels may be super important in people who can’t give up their NAD lowering habits – oxalate, metformin, alcohol, miralax, melatonin, etc.****
3. I’m NOT going to eat a lysine restricted diet because I don’t have a genetic mutation in ALDH7A1. I won’t make my clients do this either, unless they think they are toxic, because diet restriction of amino acids is too hard. If they do have this genetic mutation, though, I would. OR if they have symptoms of B6 toxicity I might recommend it.
4. Instead, work on sparing NAD because that is potentially what is causing the high pyridoxine or pipecolic acid. Low NAD may actually decrease ALDH7A1 activity. And…get this…people with liver disease have high Pipecolic acid levels. So…low NAD seen in oxalate poisoning and chronic alcohol issues leads to liver disease eventually. (4).
It’s all interconnected. How does vitamin A play into this? Excess retinol and retinal metabolism might deplete NAD in the same way. Once levels are high because of low NAD state, the vitamin A itself becomes a potential way that NAD levels are lowered. A vicious cycle.
There are no perfect solutions in nutrition and metabolism. Only trade offs. Maranatha.
I’m a dietitian. Not a doctor. Talk with your doctor or personal healthcare practitioner before you make any changes to your diet, supplements, medications, or lifestyle. This is only meant to inform, not to treat or diagnose a condition.
It seems that Vitamin A metabolism is altered by multiple factors. I have clients who have multiple medical issues that are also vitamin A toxic. It has to do with different medications that they take that also impair vitamin A metabolism. These medications include Miralax, Melatonin, H2 receptor antagonist, excess vitamin C, Metformin, and Lasix (see this post). The list continues to get longer and longer. So it seems that vitamin A metabolism is easily altered by many medications, but also diet (oxalate, aldehydes, alcohol). Detoxification of retinoic acid from the body is also altered by many factors (see this post).
SUMMARY – for those who don’t like long winded explanations.
Hydrocortisone (HC) at higher doses has a paradoxical effect on Tryptophan metabolism – This helps with mood and perceived energy
HC at higher doses causes LESS tryptophan to become niacin
Low niacin leads to low NAD
Low NAD leads to low metabolism of vitamin A from retinol and retinal (beta-carotene is a source) to retinoic acid
This means our kids are at risk for vitamin A toxicity
Vitamin A only leaves the body as retinoic acid
They also may appear to be vitamin A deficient due to low retinoic acid
Insufficient HC can also lower niacin (lower NAD) as cortisol controls the enzyme action in the first stage of Tryptophan metabolism.
Overall, kids on HC are at risk for poor vitamin A metabolism from altered NAD levels.
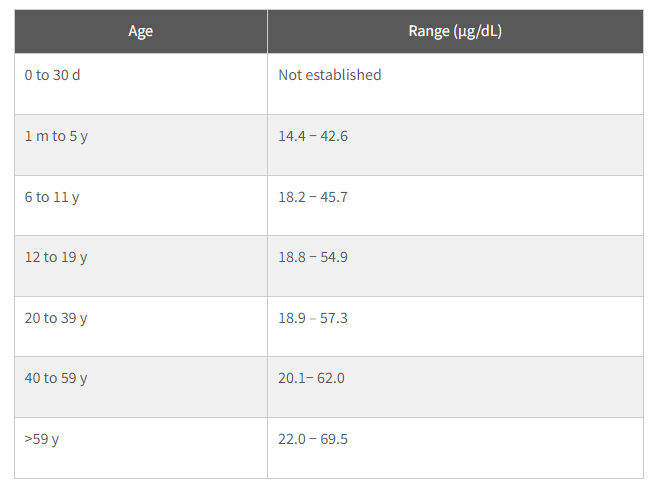
Have serum vitamin A (retinol) checked. There is a screen shot int this post of “normal” values as some labs have ridiculously high levels set.
Even if serum vitamin A levels are “normal” we don’t know how much is in our kiddos livers.
If your child is iron deficient as well, this sets them up for hepatic vitamin A toxicity because iron deficiency prevents the mobilization of vitamin A from storage.
If you are giving a niacin supplement along with HC, and your child is insanely fatigued, it could be that their tryptophan levels are WAY too high because niacin blocks the enzyme that starts the kynurenine pathway, and hydrocortisone, depending on the amount used, could also be blocking this pathway.
NORMAL SERUM VITAMIN A LEVELS BY AGE – LAB CORP. Most literature agrees that vitamin A should not be above approximately 56 ug/dl. Some laboratories set the upper limit for this test as anywhere from 90 to 120 ug/dl. Those values are way too high. https://www.labcorp.com/tests/017509/vitamin-a
Signs of poor metabolism of vitamin A (or retinol/retinal toxicity, but retinoic acid deficiency)
eczema
histamine intolerance
poor wound healing
bleeding gums
nausea
headache
high VLDL and/or LDL
insulin resistance
low platelet count (retinoic acid toxicity)
high platelet count (possible retinol toxicity symptom)
low TSH
high total T4
keratosis pilaris (chicken bump skin)
dry cracked heels
hair loss (male pattern baldness, losing eyebrows)
hypercalciuria
I’m a dietitian and I have been studying vitamin A toxicity and related metabolic pathways. Vitamin A Toxicity can occur in a low NAD state. NAD is a cofactor for enzymes that convert retinol and retinal (beta-carotene come in at retinal), to retinoic acid. NAD contains niacin. Niacin can be a supplement, but we make niacin from the amino acid tryptophan,. Approximately 95% of the Tryptophan in our body is pushed through this pathway to make niacin. The other 5% is typically used to make Serotonin.
That being said, my girls have late onset congenital adrenal hyperplasia. My 17 year old wasn’t diagnosed until 12 years old. She suffered miserably for years from eczema, allergies, and fatigue. She still does unless she “half” stress doses. She has been accused by her doctor of “over medicating”. She says that doing a half stress dose helps so much with everything! Her fatigue, her eczema, her allergies, but she is trying to be obedient to the doctor’s orders.
So, here is what I just figured out. Cortisol turns on the first enzyme in the pathway that pushes tryptophan to Niacin. If Cortisol is too low, then niacin may also be low. Paradoxically, when increasing hydrocortisone, niacin production from tryptophan goes even lower. Both corstisol deficient and over abundance of hydrocortisone can cause low production of NAD. NAD is needed to convert retinol to retinal and then into retinoic acid. When retinol is high, it causes a histamine reaction! ALLERGIES and HIVES! When retinoic acid is low it means skin can’t heal! CHRONIC ECZEMA. When retinoic acid is low, we can’t get Vitamin A out of the body. It only leaves in that form. VITAMIN A TOXICITY!
POSSIBLE HISTORY OF VITAMIN A TOXICITY WITH PROBABLE MAXED OUT LIVER STORES IN MY 17 YEAR OLD WITH NCCAH
My 17 year old was likely vitamin A toxic last year until she started stress dosing all the time because she felt bad. I say I think she was likely vitamin A toxic because her labs showed a low TSH and high retinol in the blood will cause a low TSH. Her TSH is now normal, but she is still feeling tired and fatigued. Her serum vitamin A is 39 (normal value <59 for her age). Last year she became allergic to chocolate and beans. She had to stop eating them. They are high oxalate foods that also can cause low NAD levels (see my blog for details www.weakthereforestrong.com/blog). When she stopped eating these foods, it helped increase her NAD recycling. However, I think she still has overall high vitamin A levels due to her histamine intolerance goes up and down. I think she, at times, mobilizes vitamin A quickly from stores and triggers a histamine release from mast cells. Her skin still looks terrible, too, and she has very thin blood. All signs of vitamin A toxicity.
DEFINITELY VITAMIN A TOXICITY IN MY 11 YEAR OLD WITH NCCAH
However, my 11 year old is vitamin A toxic. I think this Kynurenine pathways is part of the reason why. The other part is because we were accidentally feeding her high oxalate plantain flour. We thought it was low oxalate due to a dietitian handout that was wrong. Oxalate impairs the enzyme lactate dehydrogenase which makes NAD low resulting in vitamin A metabolism slowing down. You can read more about that on this blog, but I just realized that her NCCAH plays a HUGE role in this as well.
So, something else….this past January I was tired of my daughter using steroids to make herself feel better. Her diet is pretty limited because of foods allergies and so I decided to make her take a multivitamin. This contained vitamin A and niacin. She became even more tired and her eczema worsened. She is sleeping all day.
Hydrocortisone in higher amounts improves moved and perceived energy by lowering the Kyn:Trp ratio. This means better mood as tryptophan is made into serotonin, but also could mean lower NAD levels as well leading to poor vitamin A metabolism. This paradoxical effect of hydrocortisone needs to be explored further. I do not think it is due to steroid depletion of B6 as this would actually lead to increases in Kyn metabolites and this study found lower levels of these metabolites in those dosing with higher doses of hydrocortisone.
ORAL NIACIN, GOOD OR BAD FOR KIDS WITH CAH?
Well, when you add Niacin to the body in supplemental form. It inhibits the enzyme TDO. This essentially shuts of Tryptophan conversion to niacin, and remember, 95% of tryptophan in the body goes through this pathway, or it is made into serotonin. I think that what is happening to my daughter is that her serotonin levels are way too high because I blocked tryptophan metabolism into niacin.
Interestingly, though, this study I link to below showed an increase in tryptophan from using more hydrocortisone, which I feel is the opposite of what I would think. This actually worries me even more. This would mean that increasing doses of steroids may lead to even less niacin being made in the body! This means a low NAD state. There may be a paradoxical effect when doses are high versus low.
In any case, I think using oral niacin has pushed my daughter into an extremely high tryptophan state as she has also been stress doing. So, now we are avoiding niacin all together to see if this will help her to be able to push more tryptophan down this pathway and stop her from feeling so exhausted, and also stop her wanting to take mores steroids. I do think half stress dosing is probably worsening her NAD levels though, especially as this study shows that high dose steroids push everything back to tryptophan.
(Another important thing to note is that the supplement Nattokinase blocks the other enzyme IDO1. Taking both Niacin and Nattokinase will alter tryptophan metabolism completely. This may cause serotonin syndrome, especially in someone taking a SSRI)
CHECK KIDS ON HYDROCORTISONE FOR VITAMIN A TOXICITY
Also, I think that our kids should be checked for vitamin A toxicity. NAD is crucial for the metabolism of Retinol, Retinal, and Beta-carotene to retinoic acid. Excessive amounts of retinol in the body can cause histamine intolerance (retinol triggers mast cell histamine release), diabetes (high retinol binding protein 4), and bone loss (high retinol triggers osteoclasts to break down bone quickly leading to hypercalciuria).
High retinal levels can contribute to neurodegenerative disease and macular degeneration through combining with an ether lipid called ethanolamine making A2E. This A2E aggravates microglia cells and could be causing brain inflammation and is known to cause macular degeneration.
Low retinoic acid means poor wound healing, worsening eye sight, and poor growth. Retinoic acid is the only form of vitamin A that can leave the body. So if a person is low on NAD, they will become toxic in vitamin A.
Vitamin A is stored in the liver, until it reaches maximum capacity. After which the body will shuttle vitamin A packaged into cholesterol out of the liver in attempts to store it in adipose tissue. This makes blood cholesterol levels go up. So if your kiddo has high cholesterol, this is likely the cause.
When retinol is high, it can cause insulin resistance which will result in high triglycerides or at minimum a triglyceride:HDL ratio greater than 3.5 on labs which will indicate insulin resistance which will eventually become diabetes.
MONITORING NAD IS IMPORTANT
So it’s important for our kids to have normal NAD levels. This can be altered due to them being steroid dependent. Cortisol induces the production of niacin in the body. Adding a niacin supplement will inhibit this pathway and make them TIRED as heck, at risk for serotonin syndrome, but they may be better metabolizers of vitamin A, if they aren’t impairing their metabolism in other ways (high oxalate foods, melatonin, miralax, etc.) Maybe kids with CAH need to monitor things that lower cellular NAD levels.
I’m a dietitian, not a doctor. This post was written only to inform, and to share, because I seriously care about how our kids feel. Please consult with a physician before making any changes to medications, diet, supplements or lifestyle.
I’m a dietitian, not a doctor. This is only written to inform and is not intended to diagnose or treat a disease. Please consult with your physician prior to making any changes in medications, diet, or lifestyle.
Calling all seizure experts because I am not one. I’ve let Zoey’s “diffuse cerebral dysfunction with epileptic discharges” be unexplored because our neuro felt she wasn’t having too many epileptic discharges (her current EEG results are pending), and so medication had more risks than benefits since she does have this very slow back ground wave issue.
So, I’m not an expert in seizures, but I have a hypothesis. I propose that Zoey’s slow background waves are from low levels of ethanolamine containing ether lipids due to retinal “stealing” her ethanolamine. So structurally she is compromised pushing her towards a very slow brain.
From a biochemistry stand point, I think she fluctuates between high levels of retinoic acid and low levels of retinoic acid depending on what is going on with her mitochondrial levels of NAD. Overall, she probably has way to much vitamin A in the brain, so that adds to the fun puzzle. At any given point Zoey may have too much retinoic acid causing SLOW brain or too little retinoic acid (lots of retinal to bind ethanolamine) causing FAST brain (epileptic discharges). There are no perfect solutions in nutrition and metabolism; only trade offs.
Brain Dump Notes
Voltage gated calcium channels need to be “open” for nerves to conduct- voltage gated calcium channels need to be “closed” for nerves to stop conduction
retinoic acid helps to “close” voltage gated calcium channels-
if retinoic acid levels are too low in the brain, more voltage gated channels will be “open” leading to rapid firing of nerves (seizure)-
if retinoic acid levels are too high in the brain, then too many voltage gated channels will be “closed” leading to a very slow firing of nerves (diffuse cerebral dysfunction)
the fluctuation of retinoic acid in the brain is dependent on the enzymes ADH and ALDH as well as NAD levels- alcohol can directly tie up ADH and ALDH which would lower retinoic acid.
Alcoholics sometimes have seizures. Also, too many aldehydes in the diet could cause similar issues (people with histamine issues could be at risk as they are sensitive to acetylaldehydes which I think is really just a sign of low NAD or mitochondrial dysfunction)
a pathogenic gut microbiome can steal NAD leading to low NAD which would mean low retinoic acid levels. Low retinoic acid levels will mean more calcium channels are “open” causing seizures or possibly epileptic discharges on top of slow brain waves from low ether lipid status.
low NAD levels in the brain will cause low retinoic acid, but high retinal levels.
This causes retinal to steal ethanolamine lipids leading to A2E shift which causes microglia cells to attack and causes brain inflammation and nuerodegeneration.
Ummm….retinoic acid metabolism in the brain is apparently crucial for normal brain function. – This highlighted part of a journal that I’m reading about voltage gated calcium channels is interesting. We are still not sure what truly regulates the brain. Maybe NAD and vitamin A are part of this?
I have been longing for the tree of life that is in the book of Revelation. It has fruit each month, 12 different kinds, and the leaves are for the healing of the nation. I’m sure they are low oxalate!
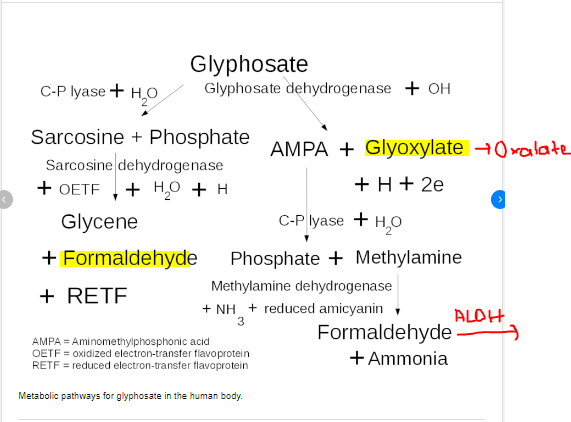
I think I figured out why the 1980-ish study found that plantain had only 1 mg of oxalate, but new data is closer to 524 mg of oxalate. It is the increased use of glyphosate. Glyphosate is not just on our fruits and vegetables that aren’t organic. It is in the soil. It can stay in the soil for many years, but decreases as plants suck it up through their root systems. Then the plants metabolize the glyphosate to….oxalate!!! They aren’t naturally poisonous. They are trying to protect themselves from glyphosate. We also metabolize glyphosate that we consume to oxalate! There are some bacteria that can eat oxalate, but most people do not have this healthy oxalobacter formenges. Maybe it died off with glyphosate increases? I think so.
In my opinion, So our heavenly Father didn’t intent for us to have this poison in our foods. I do know of one lab, Unlocked Labs, who is working on turning on genes in bacteria so that they eat oxalate. That’s interesting. I sent them the hypothesis about NAD dependent vitamin A metabolism and how oxalate is inhibiting NAD recycling. We shall see how that goes.
This is the metabolism of glyphosate in the human body. The body can make two products that cause damage to vitamin A metabolism. Oxalate and Formaldehyde. Oxalate impairs LDH causing decrease in NAD needed for retinol and retinal metabolism to retinoic acid. Formaldehyde puts burden on Aldehyde dehydrogenase that is needed for retinal to retinoic acid conversion.
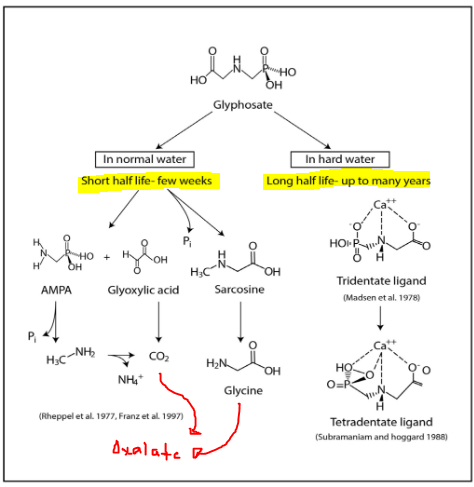
Water quality matters. This is shows that hard water (water treated with chemicals and minerals such as the water that we get from the city) will cause glyphosate to remain metabolized for many years. Normal water will result in glyphosate breaking down into metabolites that can still harm people if they are B6 or Thiamine deficienct, but it will degrade faster and not persist in the environment.
source: http://www.mdpi.com/1660-4601/11/2/2125
There’s so much more research on this persistent poison, but I think I will stop here and make some recommendations.
Avoid the dirty dozen (EWG is a good place to start)
Avoid wheat, corn, oats, and soy if not organic
Realize that the oxalate in plants is higher now likely due to the fact that glyphosate is so abundant in our soil and water supply
Forgive the dietitian who made the bad handout for not realizing this, but send her this blog.
This is a quick hypothesis on the need to correct the ability to catabolize retinoic acid (final irreversible product of vitamin A metabolism). This hypothesis is not intended to diagnose, treat, or cure a disease. It is only written for to inform. Please consult with your personal healthcare practitioner before making any changes. I am not a doctor. I am dietitian with a quirky set of skills. – Meredith Arthur, MS, RD, LD
Retinoic acid (RA) has to be catabolized and removed from the body or levels may go to high. Some symptoms that I contribute to high retinoic acid include, nausea, peeling skin, burning sensation of the skin, headaches, fatigue,
This breakdown of RA requires CYP26. There are no known inhibitors of CYP26…yet…but it does require NADPH. This can be made from NAD. In a low NAD state, you won’t have enough NADPH to be able to metabolize retinoic acid. As you work on changing habits that decrease NAD, this NADPH should improve, BUT there is a chance that you are over using all cytochrome P450 enzymes resulting in a burden on NADPH. This could lead to increased levels of RA. High RA can poison a person (think Accutane poisoning). So, I’m working on figuring out how to maximize this NADPH dependent removal of RA.
After it is metabolized by CYP26, the products of RA must go through the glucuronide pathway. There are many substrates that use this pathway. Stevia is one of them. All stevia glycosides are detoxified by this pathway. Monk fruit is also a glycoside, and so uses glucuronidation to be removed from the body. Many drugs use this pathway. So this is another possible inhibitor of properly removing retinoic acid from the body.
There is a vitamin A toxicity group on facebook that has some good information about maximizing these pathways. As I explore this more, I will add what I think is valuable information to this post. So far, these are the most important changes to make to diet (consult your healthcare provider before making changes):
increase egg yolks to four per day (Andrew Baird from the Vitamin A toxicity group recommends going slow with eggs and starting with one per day https://www.facebook.com/groups/3033243886748451/)
decrease sweeteners such as monk fruit and stevia
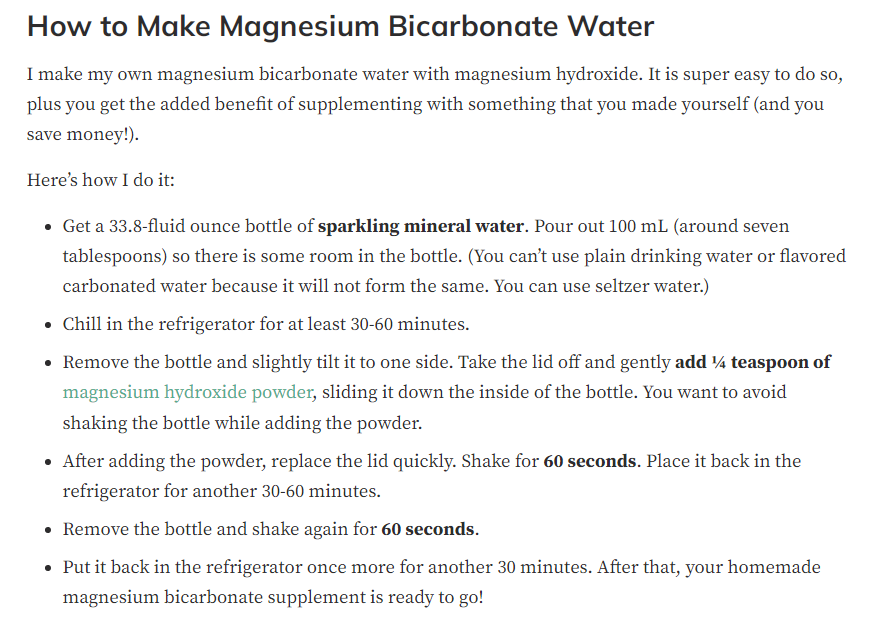
work on daily bowel movements, but not with Miralax. Magnesium bicarbonate may help as the bicarbonate also triggers mesothelial cells to make acetycholine independent of vagus nerve stimulation. Acetycholine is the major neurotransmitter of the gastrointestinal tract. I used to use Magnesium citrate with Zoey, but just yesterday one of my “treasures in heaven clients”, Meagan, told me she makes magnesium bicarbonate to increase magnesium levels. Well, I said, “You also just helped your GI tract move.” We learned from each other. Life is a team effort and God brings people together for the good of each other.
consider Taurine supplement to help with bile acid production
avoid glyphosate as this overloads cytochrome P450 and ties up NADPH in detoxifying it (Go Organic. Avoid non-organic wheat, soy, oats, corn. ) Check out EWG dirty dozen. https://www.ewg.org/foodnews/dirty-dozen.php
consider supplementation with calcium-D glucurate to support glucuronidation pathway (Thanks, Oskar for piping in on the Vitamin A toxicity group.)
DO NOT consider inositol to support the pentose phosphate shunt pathway that helps to make NADPH. I will make a post soon on why you should avoid inositol supplements in detail. However, to give a short explanation, inositol can impair the production of cardiolipin by posttranscriptional inhibition of enzymes in this pathway. I believe this production is already impaired by retinaldehyde accumulation that complexes with ethanolamine leading to A2E formation (lipofuscin). This decreases the availability of CDP diacylglycerol which is a precursor for cardiolipin. When cardiolipin levels decrease in the mitochondrial membrane, this can cause oxidative stress and cell death. Having high vitamin A status alone can cause this process by stealing a source of CDP diacylglycerol needed for cardiolipin production, but adding in inositol can completely inhibit this pathway. In fact, A2E accumulation in the eye actually causes damaged to cytochrome C oxidase leading to oxidative stress. Again…longer post coming soon.
Meagan recommends checking on Musclesandmotherhood on instagram for recipes and info about MgHCO3 https://www.instagram.com/_musclesandmotherhood/
This post was reviewed by Jenny Jones, PhD, human molecular genetics. I want to make sure that whatever I share with you has at least two critically thinking minds working on a problem. <3
This is not written to diagnose or treat a condition, but only for informative purposes. Please consult your doctor before stopping or starting medications or supplements, and before making dietary or lifestyle changes based on the information provided. – Meredith Arthur, MS, RD, LD
Now for the various ways that we can alter Vitamin A Metabolism…….
Oxalate
vitamin C (excess from supplements)
Glycine
Miralax or other PEG products
Thiamine deficiency
B6 deficiency
Iron deficiency
Zinc deficiency
H2 Receptor antagonists
High dose melatonin
Gut dysbiosis
Acetaldehyde (and alcohol)
Under each section there is a mechanism of action, followed by a possible solution. Of course, talk with your health care provider before making any changes.
OXALATE from plants or made from VITAMIN C or GLYCINE or Miralax (PEG) in the body can impair Vitamin A metabolism
Oxalate is a component of plants that is impossible for the body to completely break down. It is a poison. We absorb it at variable rates, but some of us make it in our bodies from vitamin C and glycine. Excess vitamin C becomes oxalate through direct breakdown and without enzymes. Usually this occurs in vitamin C over 2000 mg, but it can happen at lower doses as well. Never take vitamin C to “bowel tolerance” as this is likely actually death of the intestinal cells due to oxalate poisoning. Glycine is metabolized to oxalate in a B6 and thiamine deficient state, but when there is adequate B6 and Thiamine, it does not become oxalate.
When oxalate is high it impairs an enzyme called Lactate Dehydrogenase (LDH). We have to make some lactate to keep energy metabolism going. When the body is producing lactate, it also produces NAD+ which is what drives vitamin A (retinol and retinal) metabolism forward. What I found through a deep dive into literature is that Oxalate doesn’t directly inhibit alcohol dehydrogenase or retinol dehydrogenase or aldehyde dehydrogenase which was what I was searching for. Oxalate actually impairs lactate dehydrogenase (LDH) which lower NAD+ levels. I hypothesize that oxalate takes away the “energy” needed to drive those reactions forward by impairing LDH.
LDH is actually the last enzyme involved in the formation of oxalates. I believe that oxalate being able to have a feedback inhibition on LDH is a safety mechanism built into our human biology, but that it backfires and wreaks metabolic havoc on vitamin A metabolism and also energy metabolism.
Oxalate Pathogenic In Autism (Perhaps this is the connection! If oxalate impairs LDH, resulting in low NAD, then retinal levels increase. These complex with ethanolamine causing A2E and microglial activation resulting in neurological decline.)
Jenny Jones, PhD, pointed the article below out to me as supporting evidence for the connection between need for normal LDH reaction to restore NAD levels.
The article bleow is an excellent article! This gives the big picture of NAD production, recycling, and salvage pathways. Amazing! LDH, which is inhibited by oxalate, plays a pivotal role in NAD recycling.
NAD+ metabolism: pathophysiologic mechanisms and therapeutic potential
2. Avoid excess vitamin C in excess (variable per person, but most kids don’t need more than 500 mg per day)
3. Ensure adequate levels of B6 and thiamine (Seizure meds tend to deplete B6 – ask doctor about 50 mg of P5P, active form of B6) – ask doctor before starting supplements CAUTION – B6 in a low NAD state may be toxic.
4. Avoid glycine supplements and also collagen powders as these are high in glycine
MIRALAX can become OXALATE and also can tie up alcohol dehydrogenase and aldehyde dehydrogenase that are needed for Vitamin A metabolism
Approximately 3.7% of PEG based laxatives are absorbed. This can be metabolized by the body to glyoxylate and then to oxalate especially in a B6, Thiamine, or Niacin deficient state. This will impair LDH, subsequently lower NAD, and thus impair vitamin A metabolism, but also overall metabolism. In addition the first two steps of PEG metabolism involve alcohol dehydrogenase and aldehyde dehydrogenase. They are enzymes used in vitamin A metabolism. So Miralax may tie up these enzymes for an unknown period of time. This would be an interesting study in a rat lab.
So many people with Autism take PEG (Miralax). PEG can also cause gut dysbiosis (see below for info on bacterial steal of NAD+) Perhaps many have A2E complexes of the essential ether lipid ethanolamine due to increasing retinal levels (this is a hypothesis).
PEG with weights greater than 4000 aren’t absorbed (1960 studies), but somewhere along the way a manufacturer changed it out for PEG 3500, probably due to cost, and the researchers felt absorbing 200 ml out of 5400 ml was no big deal.
I propose that 3.7% absorbed of the PEG laxative are causing a big deal. And the unabsorbed product is causing gut dysbiosis.
Ever notice that the label says not for use in children? Also to not use more than a week?
2. Ask your doctor for alternatives such as magnesium, senna, glycerin suppositories, etc.
B6 DEFICIENCY
B6 deficiency can cause increased production of oxalate from the amino acid glycine. Also, thiamine is needed to activate B6 into pyridoxal-5-phosphate. In addition, B6 and thiamine deficiency can prevent the production of NAD from tryptophan. High losses of B6 can occur when oxalate clearing through the kidneys is high. B6 is also depleted by birth control. Many seizure medicines deplete B6.
Solution:
– Ask physician about taking P-5-P. (However, I believe at this time that supplementing P-5-P in a NAD deficient state due to alterations in dietary factors that prevent NAD recycling can cause B6 to become toxic. See this post for that hypothesis. CAUTION – B6 in a low NAD state may be toxic.
– Ask physician about thiamine supplementation
– Avoid glycine supplements or collagen powders which are high in glycine
Thiamine is needed to activate B6 to its P5P form. Thiamine is also needed to help pyruvate become lactate, which leads to adequate levels of NAD+. Thiamine deficiency can be caused by drinking too much coffee, tea, or caffeinated soda. It can also be depleted by the drugs lasix and metformin.
Solution:
– Talk with your doctor about thiamine supplementation (there are four forms, thiamine HCL, thiamine mononitrate, benfotiamine, and TTFD)
– Stop drinking so much caffeine!
– do not stop a medication without talking with your doctor
ZINC DEFICIENCY
Zinc is needed to metabolize vitamin A into retinoic acid. However, excess dietary zinc can cause a copper deficiency which can cause microcytic anemia and also neurological damage. Excess iron supplementation can cause zinc deficiency, so if you are on iron, then Zinc deficiency is possible.
Solution:
1. Ask your doctor to check ceruloplasmin and plasma zinc levels to evaluation zinc and copper
2. Ask your doctor about starting a Zinc:Copper Balance supplement. It should be about 10 to 15 mg of Zinc to every 1 mg of copper. THe amount of zinc and copper you need may need to be adjusted.
IRON DEFICIENCY
Iron deficiency impairs the mobilization of vitamin A from the liver. This can lead to a functional vitamin A deficiency, and excessive liver stores of vitamin A. The functional vitamin A deficiency worsens iron deficiency because retinoic acid, active vitamin A, down regulates the production of hepcidin by the liver, but also adipose tissues. Hepcidin increases. Hepcidin essentially locks iron into the cells of the intestine or liver so it can impair iron absorption, but also can lead to iron toxicity in the liver. (Never blindly supplement iron. Always ask for iron studies.)
Once liver capacity for vitamin A is reached, the body will increase cholesterol production in efforts to send vitamin A to fat cells for storage. If there is not enough choline to make cholesterol, fat will accumulate in the liver causing fatty liver disease. This can occur with or without iron deficiency. There are many other factors that contribute to poor vitamin A metabolism beyond iron deficiency.
Also, iron deficiency causes slowing of TCA cycle and build up of citrate which becomes a building block for triglyceride production. Less energy is also produced from food eaten because of this slowing of the TCA cycle that makes ATP in the body.
Sometimes iron deficiency that isn’t responding to iron supplementation is actually copper deficiency. If you have been on iron a long time, you should have your copper levels checked (ceruloplasmin) due to high dose iron supplements impair copper absorption. Once copper is low, then iron can’t be absorbed.
Vitamin A can’t be mobilized during iron deficient state
– Ask doctor to check iron studies (ferritin, transferrin, TIBC, % iron saturation)
– If iron deficiency is found, then don’t dose iron every day. This will increase hepcidin levels and because retinoic acid is low, hepcidin won’t be regulated well and iron deficiency will worsen.
– Instead ask your physician about low dose iron supplementation such as 40 mg of iron bis-glycinate every other day in the morning. Dosing in this manner will not increase hepcidin as much. This iron can also be paired with vitamin C (but not more than 250 mg) to enhance absorption.
H2 receptor antagonists have been shown to impair the conversion of retinol to retinoic acid by altering NAD+ levels in cells. One of these studies said that famotidine didn’t cause this, but another study did, and so I don’t feel comfortable with famotidine (Pepcid). Also these medications can cause iron and copper deficiency leading to iron deficiency which worsens vitamin A mobilization from the liver.
1. Wean off of H2 receptor antagonist if possible with your doctors permission
2. Possibly change to a proton pump inhibitor (although these still can cause iron and copper deficiency) **** Proton pump inhibitors actually increase ALDH enzyme activity and can lead to a rapid conversion of retinal to retinoic acid. This is something to consider if you are vitamin A toxic and have very poor detoxification pathways. This could cause retinoic acid poisoning. Symptoms would be peeling skin, blisters, headache, and nausea.**** https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9290858/
HIGH DOSE MELATONIN impairs Vitamin A metabolism
(This could pertain to individuals who take more than 5 mg per day. Also anyone who doses melatonin multiple times a day. Monitor yourself for symptoms of overdose such as headache, hypotension, hypertension, drowsiness, vomiting, alopecia.)
Melatonin overdosing is another possible mechanism by which vitamin A metabolism can be impaired. Melatonin is metabolized in the Kynuric pathway which uses the enzymes alcohol dehydrogenase and aldehyde dehydrogenase. These enzymes are also used in vitamin A metabolism. Large doses of melatonin could compete with Vitamin A for metabolism resulting in a retinoic acid deficiency. Alopecia and dermatological manifestations of melatonin overdose could actually be related to retinoic acid deficiency.
In addition, when metabolizing large amounts of melatonin, NAD is used which may contribute to low cellular levels of NAD. This can result in impaired energy (ATP) levels leading to the symptoms described in melatonin overdose such as fatigue. This could also cause buildup of lactate resulting in lactic acidosis which would account for the vomiting seen in melatonin overdose.
Solution: Don’t go over 3 mg of Melatonin per day for kids. Work with a sleep psychologist on sleep hygiene.
GUT DYSBIOSIS impairs Vitamin A metabolism
Another possible mechanism by which vitamin A metabolism can be altered is when NAD levels are low due to gut dysbiosis. It is possible for pathogenic bacteria to “steal” the NAD that is needed to metabolize vitamin A.
Solution: Start a probiotic. Preferably a well researched probiotic such as MegaSporeBiotic. I’m working with microbiome labs (MegaSporeBiotic). They know that their product lowers a toxin that is produced by bad bacteria and so it should lower NAD+ steal. It is clinically proven. However, Kara, one of their dietitians, is going to help me research other bacteria strains that they know don’t steal NAD.
FERMENTED FOODS CAN IMPAIR VITAMIN A METABOLISM
Fermented foods, tea, soda, and coffee contain acetaldehyde. Acetaldehyde metabolism uses up NAD+ resulting in less NAD+ available in the conversion of retinol and retinol to retinoic acid. It also uses alcohol dehydrogenase and aldehyde dehydrogenase that are needed for Vitamin A metabolism. Fermented food: Kefir, Kombucha, sauerkraut, yogurt, etc.
Alcohol actually causes the same problem. It uses up NAD+ and also ties up enzymes so that less vitamin A is metabolized to retinoic acid.
Interestingly, foods high in acetaldehyde are avoided on a low histamine diet because they tend to “release” histamine. Perhaps this is because retinol triggers mast cells to release histamine.
Poor metabolism of vitamin A leads to high retinal levels
Retinal can comlex with ethanolamine making A2E
microglia cells are aggravated by A2E
this increase inflammation in the brain
low ethanolamine due to binding to retinal decreases the ethanolamine needed for ether lipid synthesis
neurological function declines as retinal levels increase
The Solution (in this order)
avoid vitamin A supplementation and intake above the RDA including carotenoids as these enter at retinal level. (Carrots aren’t safe in large amounts, and having orange skin is not benign.)
increase choline to support acetycholine production, and to help with bile production needed for clearance of metabolized vitamin A
maximize CYP26 enzyme function and glucuronidation pathways through proper supplementation
improve NAD production through proper supplementation
maximize retinal/retinol metabolism by avoiding NAD disruption
This is not written to diagnose or treat a condition, but only for informative purposes. Please consult your doctor before stopping or starting medications or supplements, and before making dietary or lifestyle changes based on the information provided. – Meredith Arthur, MS, RD, LD
This is a hypothesis on nervous system manifestations of poor vitamin A metabolism There are many ways by which we can impair our ability to metabolize vitamin A through disruption of cellular ratio of NAD:NADH. Low NAD levels impair the conversion of retinol and retinal to retinoic acid. Excess retinal levels in the body may be contributing to neurological decline. I believe that this is a contributor to Autism and neurological diseases.
(For 2q23.1/MBD5 deletion group — I know that our kids have neurodevelopmental disorders, but that doesn’t mean that they can’t have other health conditions that cause brain injury. I’m checking with the Elsea lab to see if MBD5 may be modulating some of the genes that involve these pathways.)
High levels of retinal can form a complex with ethanolamine to form A2E. This may decrease levels of ethanolamine containing ether lipids which may lead to neurological decline in and of itself. Low ethanolamine levels have been found in individuals with Autism and Alzheimer’s disease.
In addition, there is evidence that A2E stimulates microglia cells of the immune system to dysfunction in the eye resulting in macular degeneration. In Alzheimer’s disease, microglia cells have been implicated in neurodegeneration. Perhaps this is by an A2E mechanism as well. Individuals with Alzheimer’s disease typically do have higher levels of retinol binding protein 4 (some retinal is converted back into retinol and can be bound to retinol binding protein).
Another intersting connection between retinal and Autism is that it has been shown that individuals with Autism have impaired aldehyde metabolism. This could be genetic in origin due to polymorphisms in genes related to alcohol and aldehyde metabolism. What if it is related to diet and drug choices. Alcohol dehydrogenase and aldehyde dehydrogenase require NAD to work properly. If individuals with Autism are consuming a high oxalate diet, they are likely impairing LDH and causing low NAD levels. This slows aldehyde metabolism.
Over the past 11 years, my daughter, Zoey, has had periods throughout the day that she walked as if she were drunk. She also suffered from what doctors wanted to diagnose as “cyclic vomiting syndrome”. Looking back, the more oxalate that she was consuming, the more ataxia I would see, and the worse gastrointestinal symptoms she would have (reflux, constipatin, nuasea, vomiting). She would also have extreme mood swings and behaviors that over the past two years that were so extreme that her neurologist recommended she be put on a “mood stabilizer”. These were only symptoms of underlying impaired ability to metabolize aldehydes and the A2E ethanolamine steal altering her autonomic nervous system function.
Oxalate was indirectly impairing her ability to metabolize alcohol and aldehydes. We actually do make these consistently during metabolism, and so any disruption in NAD will impair clearance of these by products of metabolism. There are many ways to alter NAD beyond just oxalates.
My poor girl has been drunk on her own metabolites! I wasn’t giving her sips of beer! Hahahah! And….now that I am no longer accidentally poisoning her with oxalate, she is not running into walls as much or falling as much. It must feel good to not be drunk. She also has no more nausea or vomiting, and no significant reflux.
So, there is a huge connection here between retinal metabolism and the existence of impaired aldehyde metabolism in Autism, but not just Autism….
Perhaps Alzheimer’s disease is at least in part due to impaired Vitamin A metabolism and altered aldehyde metabolism. Anger and emotional dysregulation can be a serious issue in individuals with Alzheimer’s disease.
Perhaps individuals with underlying neurodevelopmental disorders caused by genetic aberrations, are more sensitive to alterations in vitamin A metabolism which leads them down a worsening pathway of neurological decline. People with genetic syndromes should be closely monitored for impaired vitamin A metabolism.
Perhaps other psychiatric disorders such as schizophrenia, bipoloar disorder, and major depressive disorder are symptoms of impaired Vitamin A metabolism. There is literature that shows interactions between Vitamin A and these psychiatric disorders. (See studies below)
The Pivotal Role of Aldehyde Toxicity in Autism Spectrum Disorder: The Therapeutic Potential of Micronutrient Supplementation
Macular Degeneration (A2E schiff base from retinal-ethanolamine complex ) is associated with Alzheimer’s disease and here it is reported that amyloid beta is involved in this process. https://www.nature.com/articles/eye2015100
At first I thought about liquid sunflower lecithin which is a good source of choline and also ethanolamine to help with low levels. Now I caution doing this, it will increase ethanolamine levels. This may cause more damage by increasing A2E complexes while retinal is still high in the body and cause a huge flair in microglia cells
However, increasing overall choline intake is important because ethanolamine can be a precursor for choline synthesis. Low levels of choline will impair acetylcholine production. When acetylcholine is low, there will be impaired autonomic nervous system function leading to slow gut motility, GERD, constipation. The best dietary source of choline is egg yolks. Do NOT use liver without considering your total body vitamin A status. Liver is extremely high in vitamin A.
Definitely address impaired vitamin A metabolism and fix areas that you are able such as low oxalate diet, B6, thiamine, and stopping melatonin or miralax (see other blog posts). This should be AFTER increasing choline intake.
If carotenoid levels are high or your child is obsessed with high carotenoid foods like carrots, possibly go on a low carotenoid diet.
Also you may have to go on a low animal source of vitamin A diet if there is evidence of retinol toxicity. This is because retinol is converted to retinal to some degree during impairment, but also it is highly likely that as this metabolic pathway is restored, then retinal levels will increase.